

The application of precisely controlled functional electrical stimulation to the shoulder, elbow and wrist for upper limb stroke rehabilitation: a feasibility study
- PMID: 24981060
- PMCID: PMC4094280
- DOI: 10.1186/1743-0003-11-105
The application of precisely controlled functional electrical stimulation to the shoulder, elbow and wrist for upper limb stroke rehabilitation: a feasibility study
Abstract
Background: Functional electrical stimulation (FES) during repetitive practice of everyday tasks can facilitate recovery of upper limb function following stroke. Reduction in impairment is strongly associated with how closely FES assists performance, with advanced iterative learning control (ILC) technology providing precise upper-limb assistance. The aim of this study is to investigate the feasibility of extending ILC technology to control FES of three muscle groups in the upper limb to facilitate functional motor recovery post-stroke.
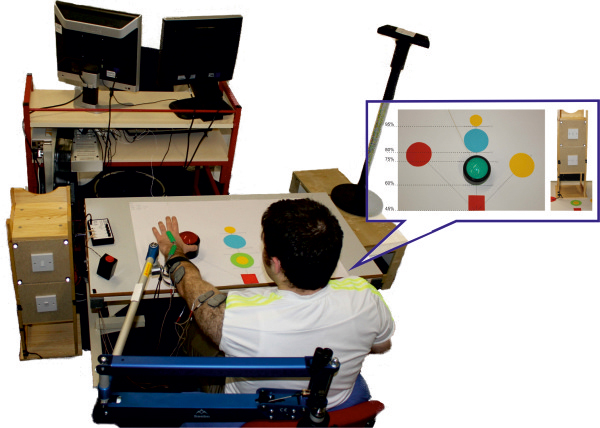
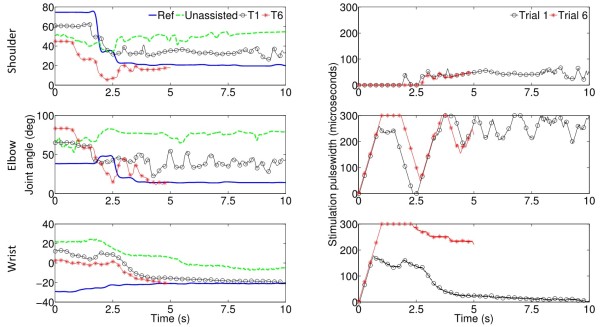
Methods: Five stroke participants with established hemiplegia undertook eighteen intervention sessions, each of one hour duration. During each session FES was applied to the anterior deltoid, triceps, and wrist/finger extensors to assist performance of functional tasks with real-objects, including closing a drawer and pressing a light switch. Advanced model-based ILC controllers used kinematic data from previous attempts at each task to update the FES applied to each muscle on the subsequent trial. This produced stimulation profiles that facilitated accurate completion of each task while encouraging voluntary effort by the participant. Kinematic data were collected using a Microsoft Kinect, and mechanical arm support was provided by a SaeboMAS. Participants completed Fugl-Meyer and Action Research Arm Test clinical assessments pre- and post-intervention, as well as FES-unassisted tasks during each intervention session.
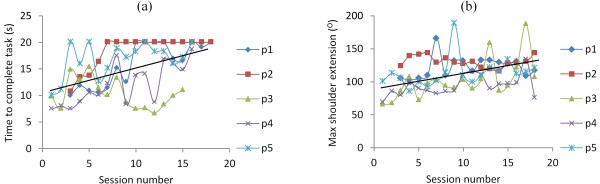
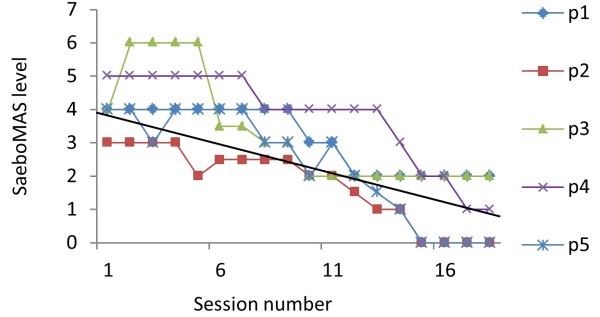
Results: Fugl-Meyer and Action Research Arm Test scores both significantly improved from pre- to post-intervention by 4.4 points. Improvements were also found in FES-unassisted performance, and the amount of arm support required to successfully perform the tasks was reduced.
Conclusions: This feasibility study indicates that technology comprising low-cost hardware fused with advanced FES controllers accurately assists upper limb movement and may reduce upper limb impairments following stroke.
Figures
References
-
- Royal College of Physicians. National Clinical Guideline for Stroke. 2012.
-
- National Audit Office Department of Health. Progress in Improving Stroke Care. 2010.
-
- Scarborough P, Peto V, Bhatnagar P, Kaur A, Leal J, Luengo-Fernandez R, Gray A, Rayner M, Allender S. Stroke statistics. British Heart Foundation Statistics Database. 2009.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
