

Neuromodulation for obsessive-compulsive disorder
- PMID: 24981434
- PMCID: PMC4121444
- DOI: 10.1007/s13311-014-0287-9
Neuromodulation for obsessive-compulsive disorder
Abstract
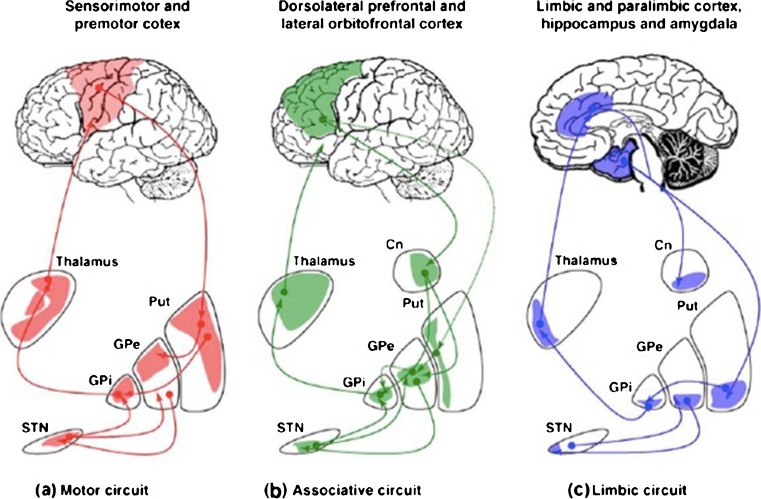
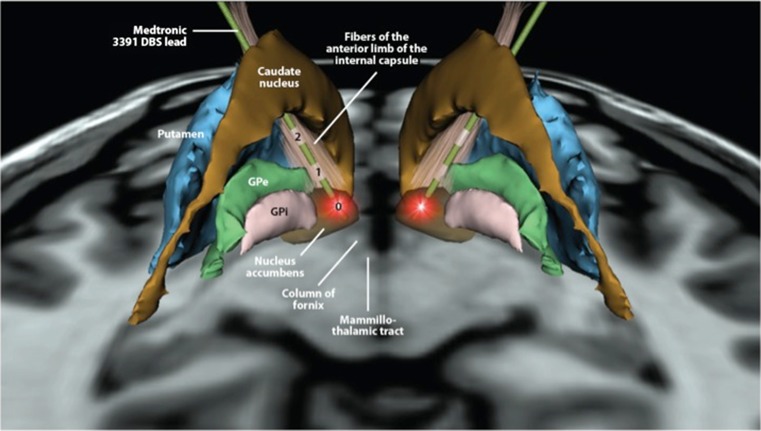
Neuromodulation shows increasing promise in the treatment of psychiatric disorders, particularly obsessive-compulsive disorder (OCD). Development of tools and techniques including deep brain stimulation, transcranial magnetic stimulation, and electroconvulsive therapy may yield additional options for patients who fail to respond to standard treatments. This article reviews the motivation for and use of these treatments in OCD. We begin with a brief description of the illness followed by discussion of the circuit models thought to underlie the disorder. These circuits provide targets for intervention. Basal ganglia and talamocortical pathophysiology, including cortico-striato-thalamo-cortical loops is a focus of this discussion. Neuroimaging findings and historical treatments that led to the use of neuromodulation for OCD are presented. We then present evidence from neuromodulation studies using deep brain stimulation, electroconvulsive therapy, and transcranial magnetic stimulation, with targets including nucleus accumbens, subthalamic nucleus inferior thalamic peduncle, dorsolateral prefrontal cortex, supplementary motor area, and orbitofrontal cortex. Finally, we explore potential future neuromodulation approaches that may further refine and improve treatment.
Figures
References
-
- Murray CJL, Lopez AD, Harvard School of Public Health., World Health Organization, World Bank. The global burden of disease: A comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Harvard School of Public Health on behalf of the World Health Organization and the World Bank, Cambridge, MA, 1996.
-
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:593–602. - PubMed
-
- American Psychiatric Association, American Psychiatric Association. Task Force on DSM-IV. Diagnostic and statistical manual of mental disorders: DSM-IV. 4th ed. American Psychiatric Association, Washington, DC, 1994.
-
- Van Ameringen M, Patterson B, Simpson W. DSM-5 obsessive-compulsive and related disorders: clinical implications of new criteria. Depress Anxiety. 2014;31:487–493. - PubMed
-
- Langston JW, Ballard P, Tetrud JW, Irwin I. Chronic Parkinsonism in humans due to a product of meperidine-analog synthesis. Science. 1983;219:979–980. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
