

Recurrence and survival outcomes after anatomic segmentectomy versus lobectomy for clinical stage I non-small-cell lung cancer: a propensity-matched analysis
- PMID: 24982447
- PMCID: PMC4121502
- DOI: 10.1200/JCO.2013.50.8762
Recurrence and survival outcomes after anatomic segmentectomy versus lobectomy for clinical stage I non-small-cell lung cancer: a propensity-matched analysis
Abstract
Purpose: Although anatomic segmentectomy has been considered a compromised procedure by many surgeons, recent retrospective, single-institution series have demonstrated tumor recurrence and patient survival rates that approximate those achieved by lobectomy. The primary objective of this study was to use propensity score matching to compare outcomes after these anatomic resection approaches for stage I non-small-cell lung cancer.
Patients and methods: A retrospective data set including 392 segmentectomy patients and 800 lobectomy patients was used to identify matched segmentectomy and lobectomy cohorts (n = 312 patients per group) using a propensity score matching algorithm that accounted for confounding effects of preoperative patient variables. Primary outcome variables included freedom from recurrence and overall survival. Factors affecting survival were assessed by Cox regression analysis and Kaplan-Meier estimates.
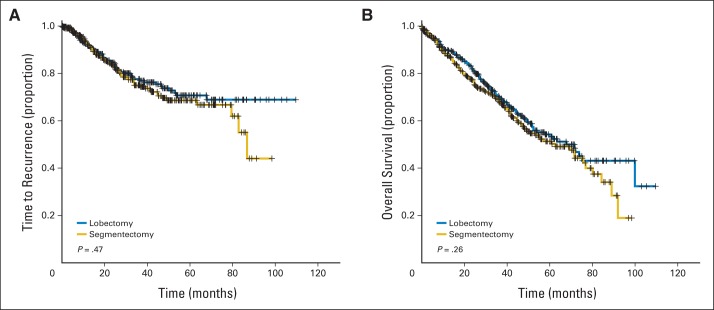
Results: Perioperative mortality was 1.2% in the segmentectomy group and 2.5% in the lobectomy group (P = .38). At a mean follow-up of 5.4 years, comparing segmentectomy with lobectomy, no differences were noted in locoregional (5.5% v 5.1%, respectively; P = 1.00), distant (14.8% v 11.6%, respectively; P = .29), or overall recurrence rates (20.2% v 16.7%, respectively; P = .30). Furthermore, when comparing segmentectomy with lobectomy, no significant differences were noted in 5-year freedom from recurrence (70% v 71%, respectively; P = .467) or 5-year survival (54% v 60%, respectively; P = .258). Segmentectomy was not found to be an independent predictor of recurrence (hazard ratio, 1.11; 95% CI, 0.87 to 1.40) or overall survival (hazard ratio, 1.17; 95% CI, 0.89 to 1.52).
Conclusion: In this large propensity-matched comparison, lobectomy was associated with modestly increased freedom from recurrence and overall survival, but the differences were not statistically significant. These results will need further validation by prospective, randomized trials (eg, Cancer and Leukemia Group B 140503 trial).
© 2014 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Role of limited sublobar resection for early-stage lung cancer: steady progress.J Clin Oncol. 2014 Aug 10;32(23):2403-4. doi: 10.1200/JCO.2014.56.4203. Epub 2014 Jun 30. J Clin Oncol. 2014. PMID: 24982454 No abstract available.
References
-
- Ginsberg RJ, Rubinstein LV Lung Cancer Study Group. Randomized trial of lobectomy versus limited resection for T1N0 non-small cell lung cancer. Ann Thorac Surg. 1995;60:615–622. - PubMed
-
- Pettiford BL, Schuchert MJ, Santos R, et al. Role of sublobar resection (segmentectomy and wedge resection) in the surgical management of non-small cell lung cancer. Thorac Surg Clin. 2007;17:175–190. - PubMed
-
- Lewis RJ. The role of video-assisted thoracic surgery for carcinoma of the lung: Wedge resection to lobectomy by simultaneous individual stapling. Ann Thorac Surg. 1993;56:762–768. - PubMed
-
- Whitson BA, Groth SS, Andrade RS, et al. Survival after lobectomy versus segmentectomy for stage I non-small cell lung cancer: A population-based analysis. Ann Thorac Surg. 2011;92:1943–1950. - PubMed
-
- Mery CM, Pappas AN, Bueno R, et al. Similar long-term survival of elderly patients with non-small cell lung cancer treated with lobectomy or wedge resection within the surveillance, epidemiology, and end results database. Chest. 2005;128:237–245. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
