

Molecular profiling and clinical outcome of high-grade serous ovarian cancer presenting with low- versus high-volume ascites
- PMID: 24982872
- PMCID: PMC4055662
- DOI: 10.1155/2014/367103
Molecular profiling and clinical outcome of high-grade serous ovarian cancer presenting with low- versus high-volume ascites
Abstract
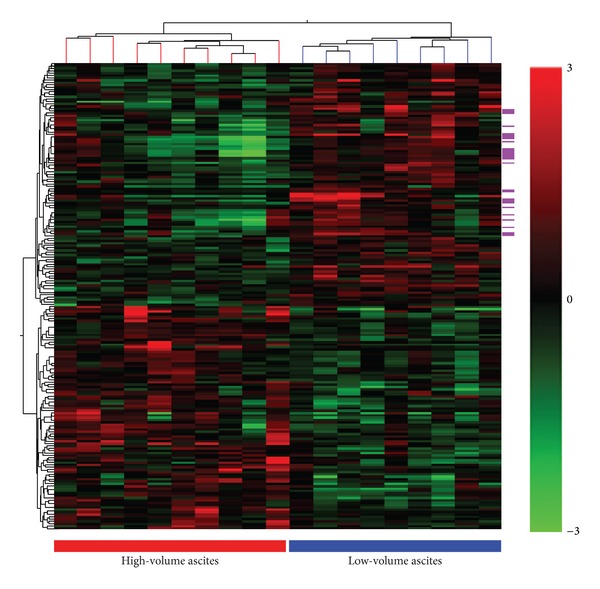
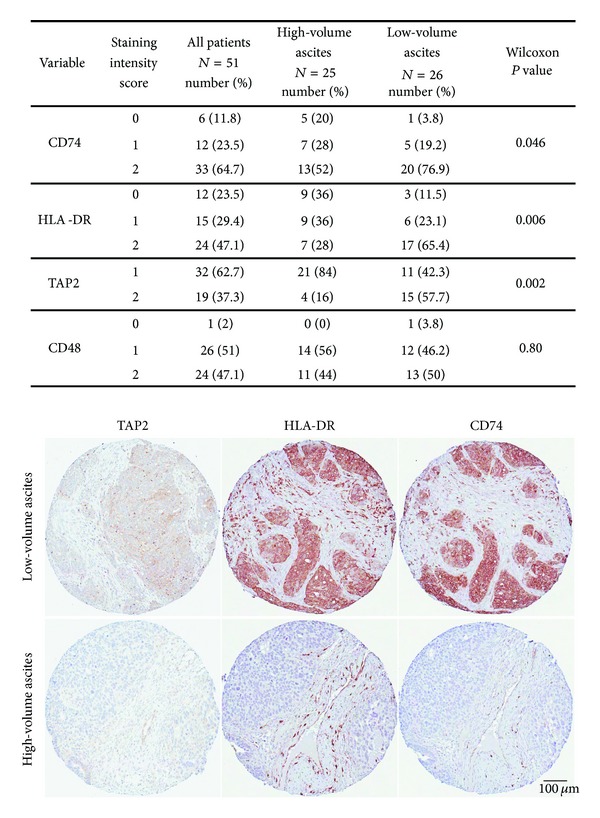
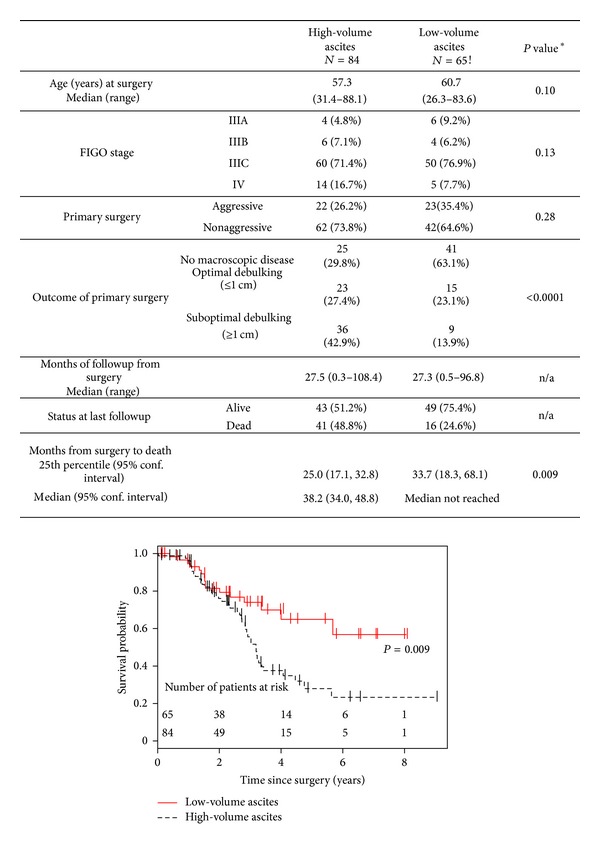
Epithelial ovarian cancer consists of multiple histotypes differing in etiology and clinical course. The most prevalent histotype is high-grade serous ovarian cancer (HGSOC), which often presents at an advanced stage frequently accompanied with high-volume ascites. While some studies suggest that ascites is associated with poor clinical outcome, most reports have not differentiated between histological subtypes or tumor grade. We compared genome-wide gene expression profiles from a discovery cohort of ten patients diagnosed with stages III-IV HGSOC with high-volume ascites and nine patients with low-volume ascites. An upregulation of immune response genes was detected in tumors from patients presenting with low-volume ascites relative to those with high-volume ascites. Immunohistochemical studies performed on tissue microarrays confirmed higher expression of proteins encoded by immune response genes and increased tumorinfiltrating cells in tumors associated with low-volume ascites. Comparison of 149 advanced-stage HGSOC cases with differential ascites volume at time of primary surgery indicated low-volume ascites correlated with better surgical outcome and longer overall survival. These findings suggest that advanced stage HGSOC presenting with low-volume ascites reflects a unique subgroup of HGSOC, which is associated with upregulation of immune related genes, more abundant tumor infiltrating cells and better clinical outcomes.
Figures
References
-
- Sankaranarayanan R, Ferlay J. Worldwide burden of gynaecological cancer: the size of the problem. Best Practice and Research: Clinical Obstetrics and Gynaecology. 2006;20(2):207–225. - PubMed
-
- Birrer MJ. The origin of ovarian cancer—is it getting clearer? The New England Journal of Medicine. 2010;363(16):1574–1575. - PubMed
-
- Tothill RW, Tinker AV, George J, et al. Novel molecular subtypes of serous and endometrioid ovarian cancer linked to clinical outcome. Clinical Cancer Research. 2008;14(16):5198–5208. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
