

Near-infrared fluorescent cholangiography facilitates identification of biliary anatomy during laparoscopic cholecystectomy
- PMID: 24986018
- PMCID: PMC4415528
- DOI: 10.1007/s00464-014-3677-5
Near-infrared fluorescent cholangiography facilitates identification of biliary anatomy during laparoscopic cholecystectomy
Abstract
Background: Intraoperative cholangiography (IOC) is the current gold standard for biliary imaging during laparoscopic cholecystectomy (LC). However, utilization of IOC remains low. Near-infrared fluorescence cholangiography (NIRF-C) is a novel, noninvasive method for real-time, intraoperative biliary mapping. Our aims were to assess the safety and efficacy of NIRF-C for identification of biliary anatomy during LC.
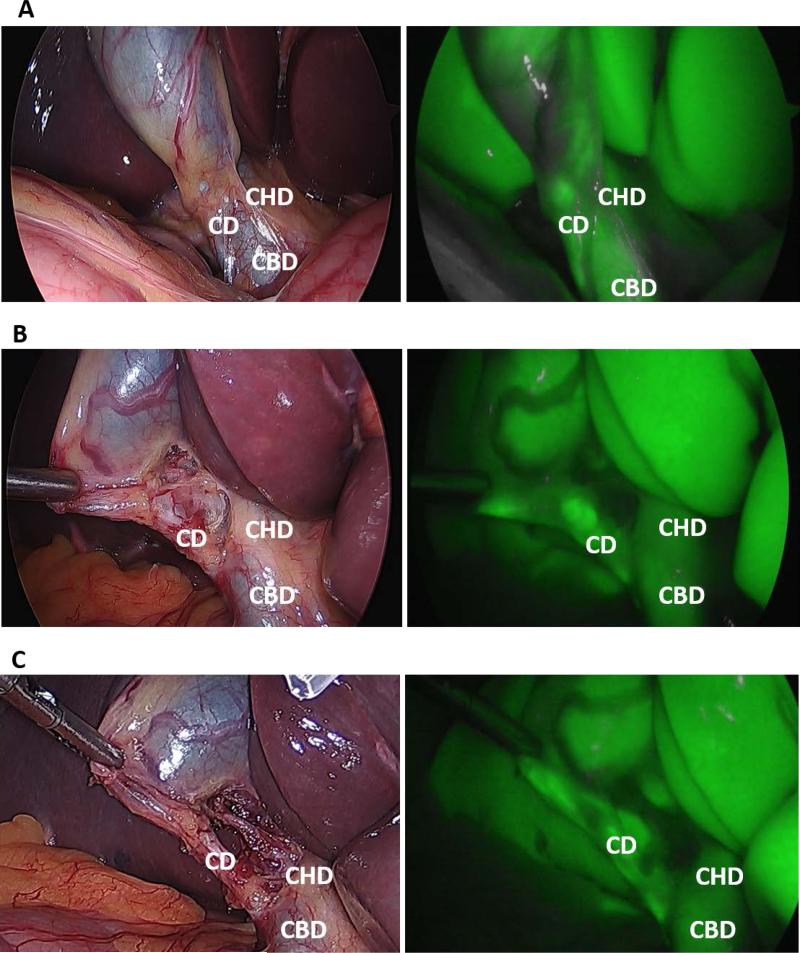
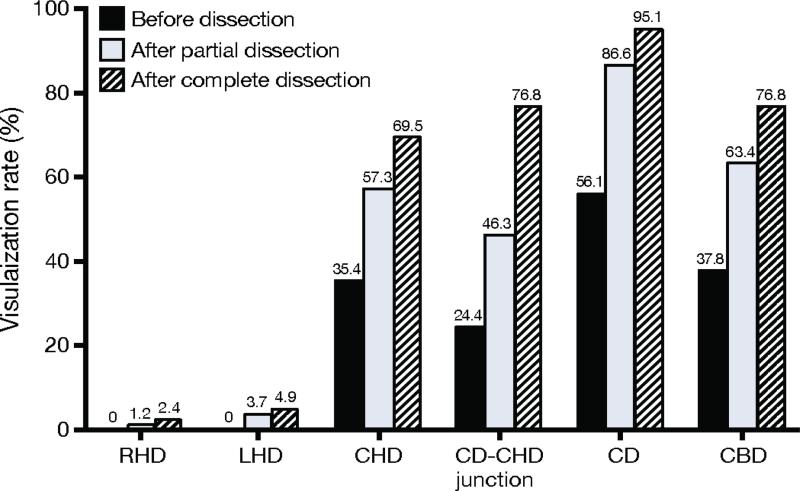
Methods: Patients were administered indocyanine green (ICG) prior to surgery. NIRF-C was used to identify extrahepatic biliary structures before and after partial and complete dissection of Calot's triangle. Routine IOC was performed in each case. Identification of biliary structures using NIRF-C and IOC, and time required to complete each procedure were collected.
Results: Eighty-two patients underwent elective LC with NIRF-C and IOC. Mean age and body mass index (BMI) were 42.6 ± 13.7 years and 31.5 ± 8.2 kg/m(2), respectively. ICG was administered 73.8 ± 26.4 min prior to incision. NIRF-C was significantly faster than IOC (1.9 ± 1.7 vs. 11.8 ± 5.3 min, p < 0.001). IOC was unobtainable in 20 (24.4 %) patients while NIRF-C did not visualize biliary structures in 4 (4.9 %) patients. After complete dissection, the rates of visualization of the cystic duct, common bile duct, and common hepatic duct using NIRF-C were 95.1, 76.8, and 69.5 %, respectively, compared to 72.0, 75.6, and 74.3 % for IOC. In 20 patients where IOC could not be obtained, NIRF-C successfully identified biliary structures in 80 % of the cases. Higher BMI was not a deterrent to visualization of anatomy with NIRF-C. No adverse events were observed with NIRF-C.
Conclusions: NIRF-C is a safe and effective alternative to IOC for imaging extrahepatic biliary structures during LC. This technique should be evaluated further under a variety of acute and chronic gallbladder inflammatory conditions to determine its usefulness in biliary ductal identification.
Figures
References
-
- Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA. 2003;289:1639–1644. - PubMed
-
- Waage A, Nilsson M. Iatrogenic bile duct injury: a population-based study of 152 776 cholecystectomies in the Swedish Inpatient Registry. Arch Surg. 2006;141:1207–1213. - PubMed
-
- Nuzzo G, Giuliante F, Giovannini I, Ardito F, D'Acapito F, Vellone M, Murazio M, Capelli G. Bile duct injury during laparoscopic cholecystectomy: results of an Italian national survey on 56 591 cholecystectomies. Arch Surg. 2005;140:986–992. - PubMed
-
- Flum DR, Cheadle A, Prela C, Dellinger EP, Chan L. Bile duct injury during cholecystectomy and survival in medicare beneficiaries. JAMA. 2003;290:2168–2173. - PubMed
-
- Adamsen S, Hansen OH, Funch-Jensen P, Schulze S, Stage JG, Wara P. Bile duct injury during laparoscopic cholecystectomy: a prospective nationwide series. J Am Coll Surg. 1997;184:571–578. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
