

Center-level variation in infection rates after coronary artery bypass grafting
- PMID: 24987052
- PMCID: PMC4130223
- DOI: 10.1161/CIRCOUTCOMES.113.000770
Center-level variation in infection rates after coronary artery bypass grafting
Abstract
Background: Health-care-acquired infections (HAIs) are a leading cause of morbidity and mortality after cardiac surgery. Prior work has identified several patient-related risk factors associated with HAIs. We hypothesized that rates of HAIs would differ across institutions, in part attributed to differences in case mix.
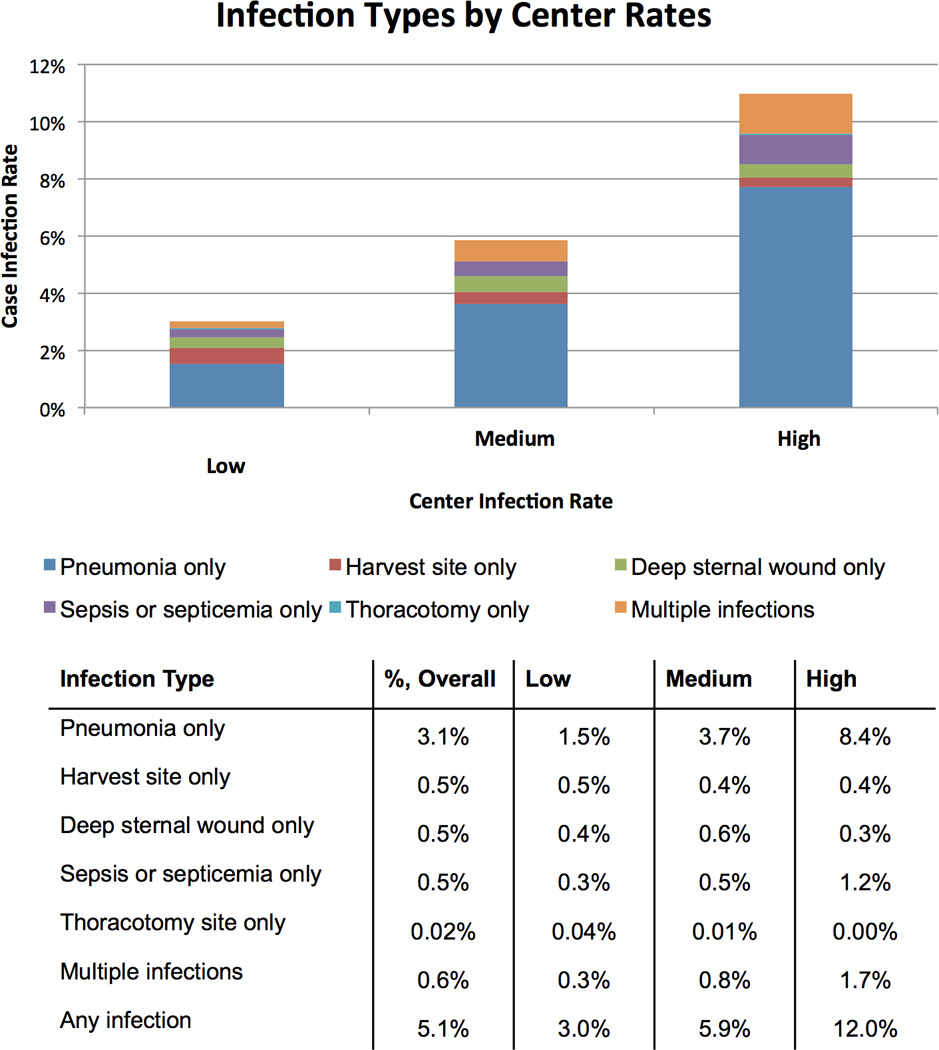
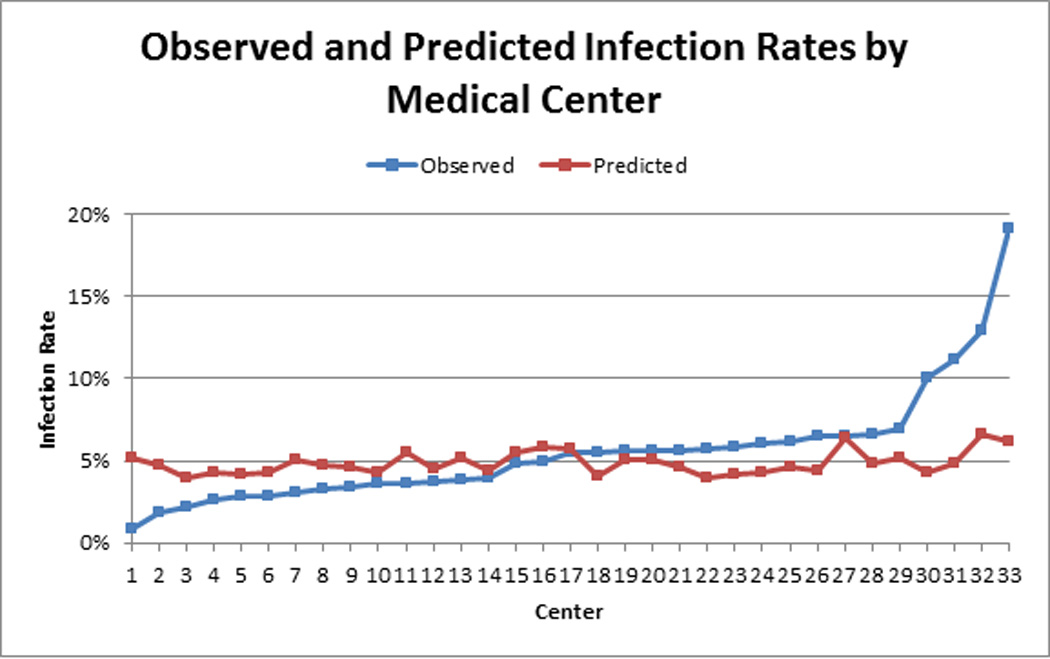
Methods and results: We analyzed 20 896 patients undergoing isolated coronary artery bypass grafting surgery at 33 medical centers in Michigan between January 1, 2009, and June 30, 2012. Overall HAIs included pneumonia, sepsis/septicemia, and surgical site infections, including deep sternal wound, thoracotomy, and harvest/cannulation site infections. We excluded patients presenting with endocarditis. Predicted rates of HAIs were estimated using multivariable logistic regression. Overall rate of HAI was 5.1% (1071 of 20 896; isolated pneumonia, 3.1% [n=644]; isolated sepsis/septicemia, 0.5% [n=99]; isolated deep sternal wound infection, 0.5% [n=96]; isolated harvest/cannulation site, 0.5% [n=97]; isolated thoracotomy, 0.02% [n=5]; multiple infections, 0.6% [n=130]). HAI subtypes differed across strata of center-level HAI rates. Although predicted risk of HAI differed in absolute terms by 2.8% across centers (3.9-6.7%; min:max), observed rates varied by 18.2% (0.9-19.1%).
Conclusions: There was a 18.2% difference in observed HAI rates across medical centers among patients undergoing isolated coronary artery bypass grafting surgery. This variability could not be explained by patient case mix. Future work should focus on the impact of other factors (eg, organizational and systems of clinical care) on risk of HAIs.
Keywords: cardiopulmonary bypass; infection; surgery.
© 2014 American Heart Association, Inc.
Figures
References
-
- Fowler VG, Jr, O'Brien SM, Muhlbaier LH, Corey GR, Ferguson TB, Peterson ED. Clinical predictors of major infections after cardiac surgery. Circulation. 2005;112:I358–I365. - PubMed
-
- Braxton JH, Marrin CA, McGrath PD, Ross CS, Morton JR, Norotsky M, Charlesworth DC, Lahey SJ, Clough RA, O'Connor GT. Northern New England Cardiovascular Disease Study Group. Mediastinitis and long-term survival after coronary artery bypass graft surgery. Ann Thorac Surg. 2000;70:2004–2007. - PubMed
-
- Brown PP, Kugelmass AD, Cohen DJ, Reynolds MR, Culler SD, Dee AD, Simon AW. The frequency and cost of complications associated with coronary artery bypass grafting surgery: Results from the United States Medicare Program. Ann Thorac Surg. 2008;85:1980–1986. - PubMed
-
- Speir AM, Kasirajan V, Barnett SD, Fonner E., Jr Additive costs of postoperative complications for isolated coronary artery bypass grafting patients in Virginia. Ann Thorac Surg. 2009;88:40–45. discussion 45–46. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
