

p53MVA therapy in patients with refractory gastrointestinal malignancies elevates p53-specific CD8+ T-cell responses
- PMID: 24987057
- PMCID: PMC4155000
- DOI: 10.1158/1078-0432.CCR-13-3361
p53MVA therapy in patients with refractory gastrointestinal malignancies elevates p53-specific CD8+ T-cell responses
Erratum in
-
Correction: p53MVA Therapy in Patients with Refractory Gastrointestinal Malignancies Elevates p53-Specific CD8+ T-cell Responses.Clin Cancer Res. 2017 Jan 1;23(1):322. doi: 10.1158/1078-0432.CCR-16-2555. Clin Cancer Res. 2017. PMID: 28049162 No abstract available.
Abstract
Purpose: To conduct a phase I trial of a modified vaccinia Ankara (MVA) vaccine delivering wild-type human p53 (p53MVA) in patients with refractory gastrointestinal cancers.
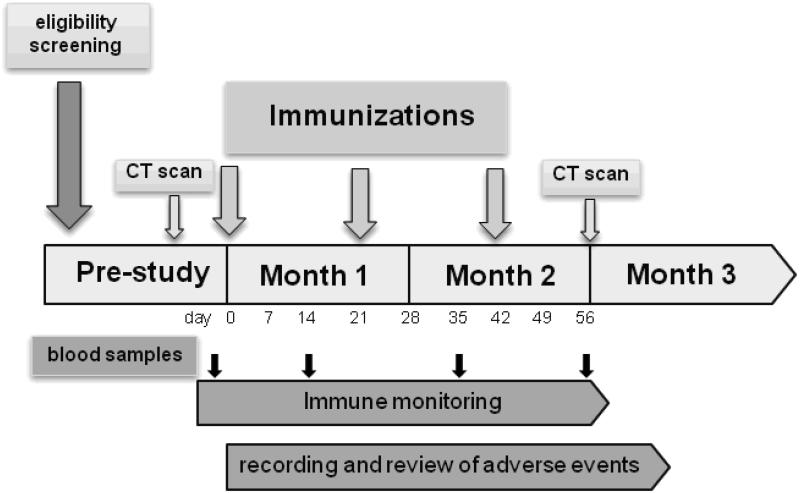
Experimental design: Three patients were vaccinated with 1.0×10(8) plaque-forming unit (pfu) p53MVA followed by nine patients at 5.6×10(8) pfu. Toxicity was classified using the NCI Common Toxicity Criteria and clinical responses were assessed by CT scan. Peripheral blood samples were collected pre- and post-immunization for immunophenotyping, monitoring of p53MVA-induced immune response, and examination of PD1 checkpoint inhibition in vitro.
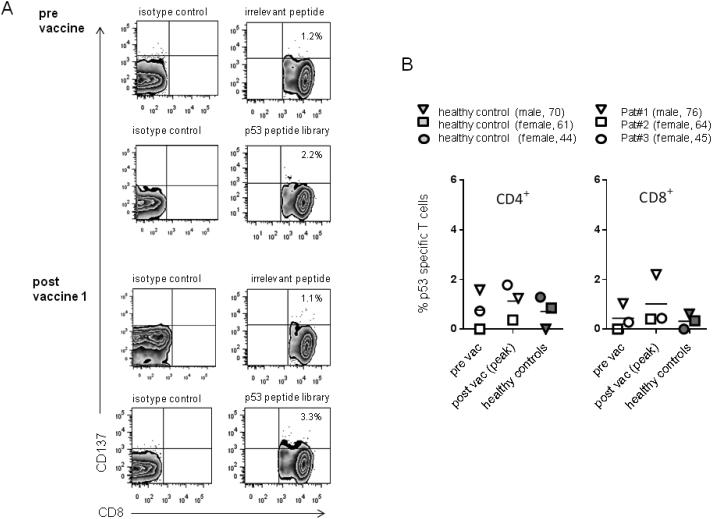
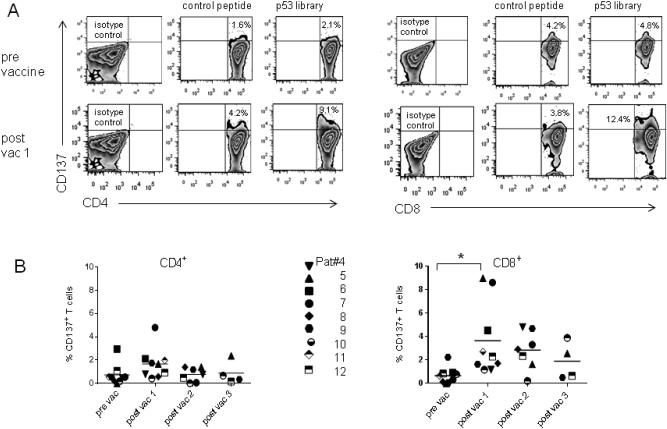
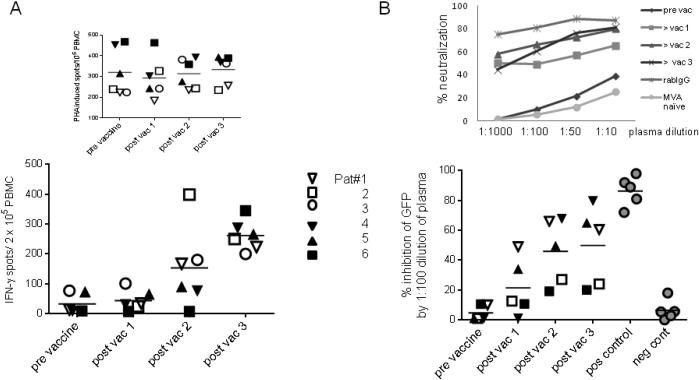
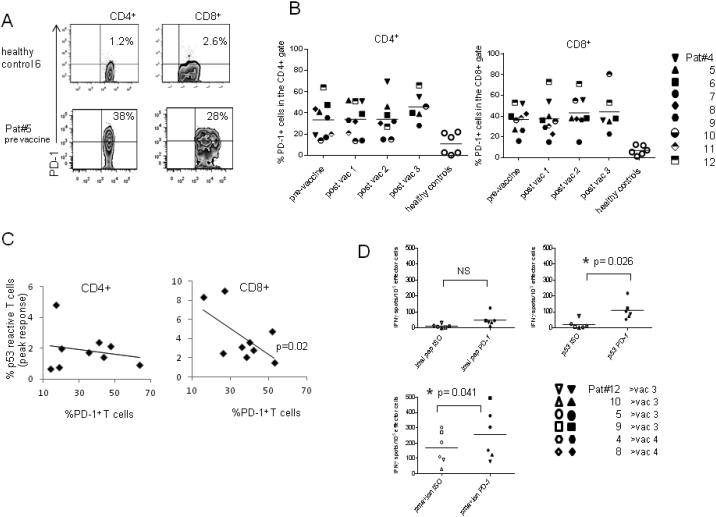
Results: p53MVA immunization was well tolerated at both doses, with no adverse events above grade 2. CD4+ and CD8+ T cells showing enhanced recognition of a p53 overlapping peptide library were detectable after the first immunization, particularly in the CD8+ T-cell compartment (P=0.03). However, in most patients, this did not expand further with the second and third immunization. The frequency of PD1+ T cells detectable in patients' peripheral blood mononuclear cells (PBMC) was significantly higher than in healthy controls. Furthermore, the frequency of PD1+ CD8+ T cells showed an inverse correlation with the peak CD8+ p53 response (P=0.02) and antibody blockade of PD1 in vitro increased the p53 immune responses detected after the second or third immunizations. Induction of strong T-cell and antibody responses to the MVA backbone were also apparent.
Conclusion: p53MVA was well tolerated and induced robust CD8+ T-cell responses. Combination of p53MVA with immune checkpoint inhibition could help sustain immune responses and lead to enhanced clinical benefit.
©2014 American Association for Cancer Research.
Figures
References
-
- Katz SC, Donkor C, Glasgow K, Pillarisetty VG, Gonen M, Espat NJ, et al. T cell infiltrate and outcome following resection of intermediate-grade primary neuroendocrine tumours and liver metastases. HPB : the official journal of the International Hepato Pancreato Biliary Association. 2010;12:674–83. - PMC - PubMed
-
- Cheever MA, Higano C. PROVENGE (Sipuleucel-T) in Prostate Cancer: The First FDA Approved Therapeutic Cancer Vaccine. Clin Cancer Res. 2011;17:3520–6. - PubMed
-
- Hodi FS. Overcoming immunological tolerance to melanoma: Targeting CTLA-4. Asia Pac J Clin Oncol. 2010;6(Suppl 1):S16–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
