

Comparative efficacy of biologics as monotherapy and in combination with methotrexate on patient reported outcomes (PROs) in rheumatoid arthritis patients with an inadequate response to conventional DMARDs--a systematic review and network meta-analysis
- PMID: 24988902
- PMCID: PMC4101713
- DOI: 10.1186/1477-7525-12-102
Comparative efficacy of biologics as monotherapy and in combination with methotrexate on patient reported outcomes (PROs) in rheumatoid arthritis patients with an inadequate response to conventional DMARDs--a systematic review and network meta-analysis
Abstract
Objective: To compare biologics as monotherapy or in combination with methotrexate (MTX) in terms of patient reported outcomes (PROs) in RA patients with an inadequate response to conventional DMARDs (DMARD-IR).
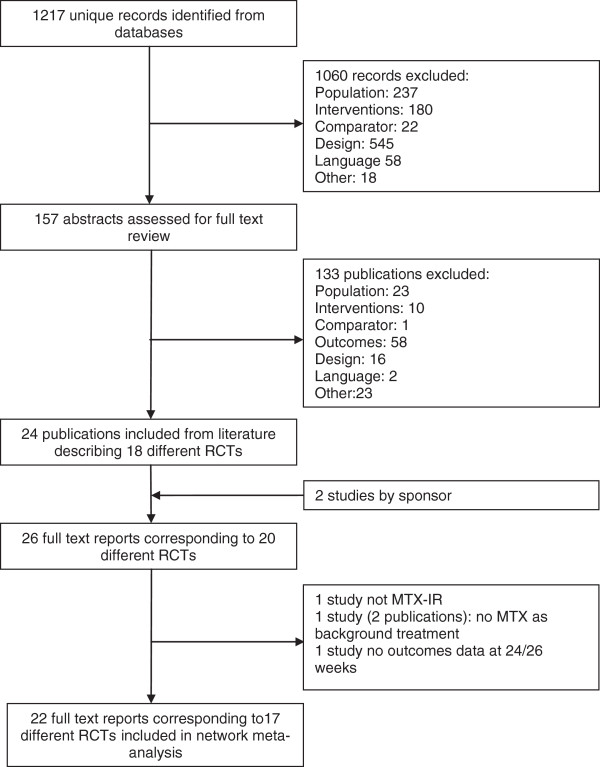
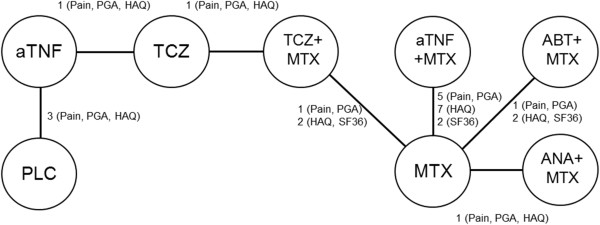
Methods: With a systematic literature review 17 RCTs were identified that evaluated adalimumab, certolizumab pegol, etanercept, golimumab, infliximab, abatacept, anakinra or tocilizumab. Treatment effects in terms of pain (0-100 mm), patient's global assessment of disease activity (PGA; 0-100 mm), Health Assessment-Questionnaire (HAQ) disability index (DI; 0-3), and the physical component summary (PCS) of the SF36 Health Survey (0-100) at 24 weeks were combined by means of Bayesian network meta-analyses.
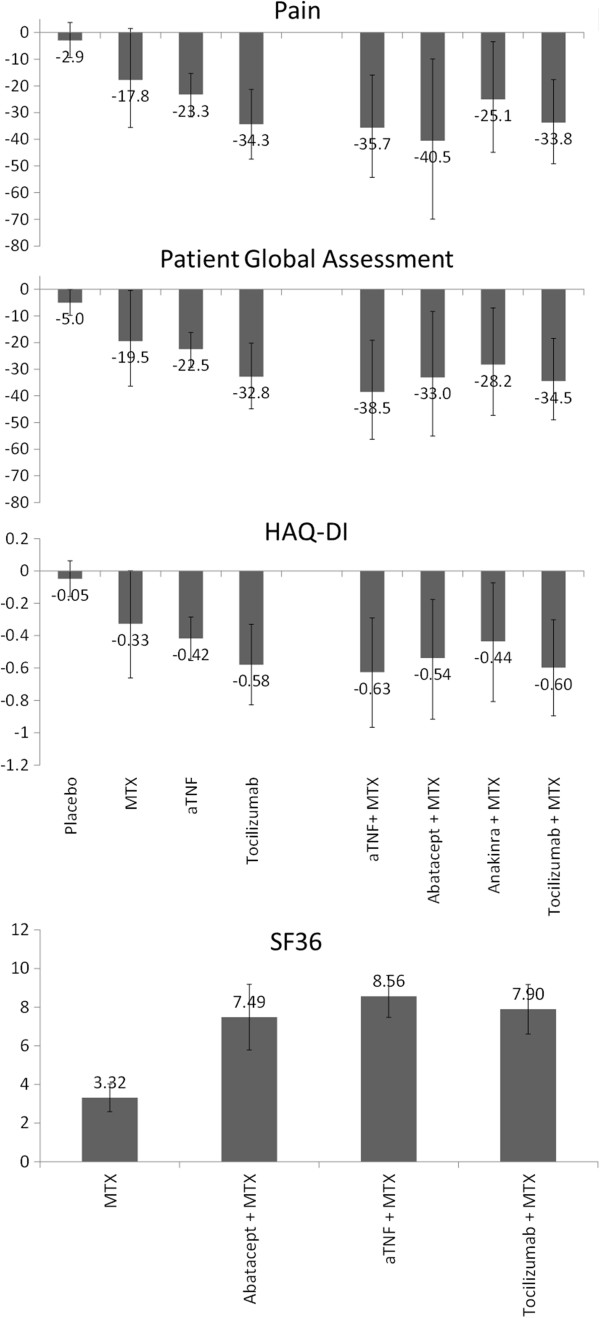
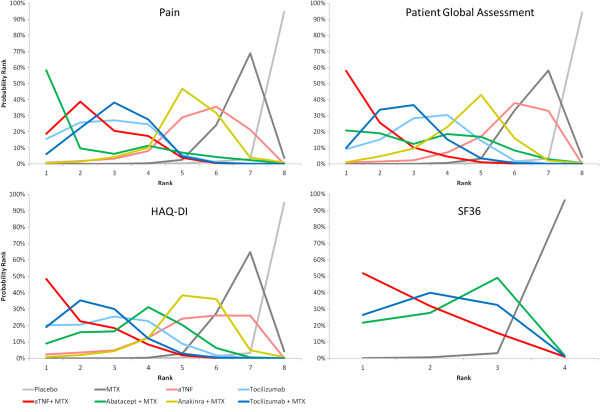
Results: With tocilizumab monotherapy, greater improvements in pain (difference = -11.1; (95% Credible Interval -21.3, -0.1)) and PGA (-10.3 (-20.4, 0.8)) were observed than with aTNF monotherapy. Tocilizumab was at least as efficacious as aTNF in HAQ-DI improvements (-0.16; (-0.37, 0.05)). aTNF + MTX (-17.9 (-23.1, -13.0) & -19.1 (-24.2, -14.4)), abatacept + MTX (-23.0 (-47.3, 1. 5) & -13.6 (-28.4, 2.0)) and tocilizumab + MTX (-16.0 (-26.3, -6.3) & -15.1 (-25.1, -5.7)) showed comparable reductions in pain and PGA relative to MTX. Efficacy of anakinra + MTX was much smaller as compared to other biologics. The greatest improvements in HAQ-DI relative to MTX were observed with aTNF + MTX (-0.30 (-0.37, -0.22)) and tocilizumab + MTX (-0.27 (-0.42, -0.12)), followed by abatacept + MTX (-0.21 (-0.37, -0.05)) and anakinra + MTX (-0.11 (-0.26, 0.05)). The improvements in SF36-PCS with abatacept + MTX, aTNF + MTX and tocilizumab + MTX were comparable. There is a >90% probability that aTNF + MTX results in a greater improvement in pain (-12.4), PGA (-16.1) and HAQ-DI (-0.21) than aTNF as monotherapy. Efficacy of tocilizumab + MTX showed comparable improvements in PROs as tocilizumab monotherapy.
Conclusions: Based on a network meta-analysis involving indirect comparison of trial findings, the following observations were made for DMARD-IR patients. In monotherapy, tocilizumab was associated with a greater improvement in pain and self-reported disease activity than aTNF, and was at least as efficacious regarding functional ability. The improvements in PROs with aTNF, abatacept and tocilizumab in combination with MTX were comparable. Improvements in PROs with tocilizumab as monotherapy were similar to that of tocilizumab + MTX, whereas aTNF as monotherapy was likely to be less efficacious than aTNF + MTX.
Figures
References
-
- Whalley D, McKenna SP, de Jong Z, van der Heijde D. Quality of life in rheumatoid arthritis. Br J Rheumatol. 1997;36:884–888. - PubMed
-
- Cole JC, Motivala SJ, Khanna D, Lee JY, Paulus HE, Irwin MR. Validation of single-factor structure and scoring protocol for the Health Assessment Questionnaire-Disability Index. Arthritis Rheum. 2005;53:536–542. - PubMed
-
- Saag KG, Teng GG, Patkar NM, Anuntiyo J, Finney C, Curtis JR, Paulus HE, Mudano A, Pisu M, Elkins-Melton M, Outman R, Allison JJ, Suarez Almazor M, Bridges SL Jr, Chatham WW, Hochberg M, MacLean C, Mikuls T, Moreland LW, O'Dell J, Turkiewicz AM, Furst DE. American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease-modifying antirheumatic drugs in rheumatoid arthritis. Arthritis Rheum. 2008;59:762–784. - PubMed
-
- Luqmani R, Hennell S, Estrach C, Basher D, Birrell F, Bosworth A, Burke F, Callaghan C, Candal-Couto J, Fokke C, Goodson N, Homer D, Jackman J, Jeffreson P, Oliver S, Reed M, Sanz L, Stableford Z, Taylor P, Todd N, Warburton L, Washbrook C, Wilkinson M. British Society for Rheumatology. British Society for Rheumatology and British Health Professionals in Rheumatology guideline for the management of rheumatoid arthritis (after the first 2 years) Rheumatology (Oxford) 2009;48:436–439. - PubMed
-
- Felson DT, Anderson JJ, Boers M, Bombardier C, Chernoff M, Fried B, Furst D, Goldsmith C, Kieszak S, Lightfoot R. The American College of Rheumatology preliminary core set of disease activity measures for rheumatoid arthritis clinical trials. The Committee on Outcome Measures in Rheumatoid Arthritis Clinical Trials. Arthritis Rheum. 1993;36:729–740. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
