

How accurately can the peak skin dose in fluoroscopy be determined using indirect dose metrics?
- PMID: 24989391
- PMCID: PMC4105961
- DOI: 10.1118/1.4884020
How accurately can the peak skin dose in fluoroscopy be determined using indirect dose metrics?
Abstract
Purpose: Skin dosimetry is important for fluoroscopically-guided interventions, as peak skin doses (PSD) that result in skin reactions can be reached during these procedures. There is no consensus as to whether or not indirect skin dosimetry is sufficiently accurate for fluoroscopically-guided interventions. However, measuring PSD with film is difficult and the decision to do so must be madea priori. The purpose of this study was to assess the accuracy of different types of indirect dose estimates and to determine if PSD can be calculated within ± 50% using indirect dose metrics for embolization procedures.
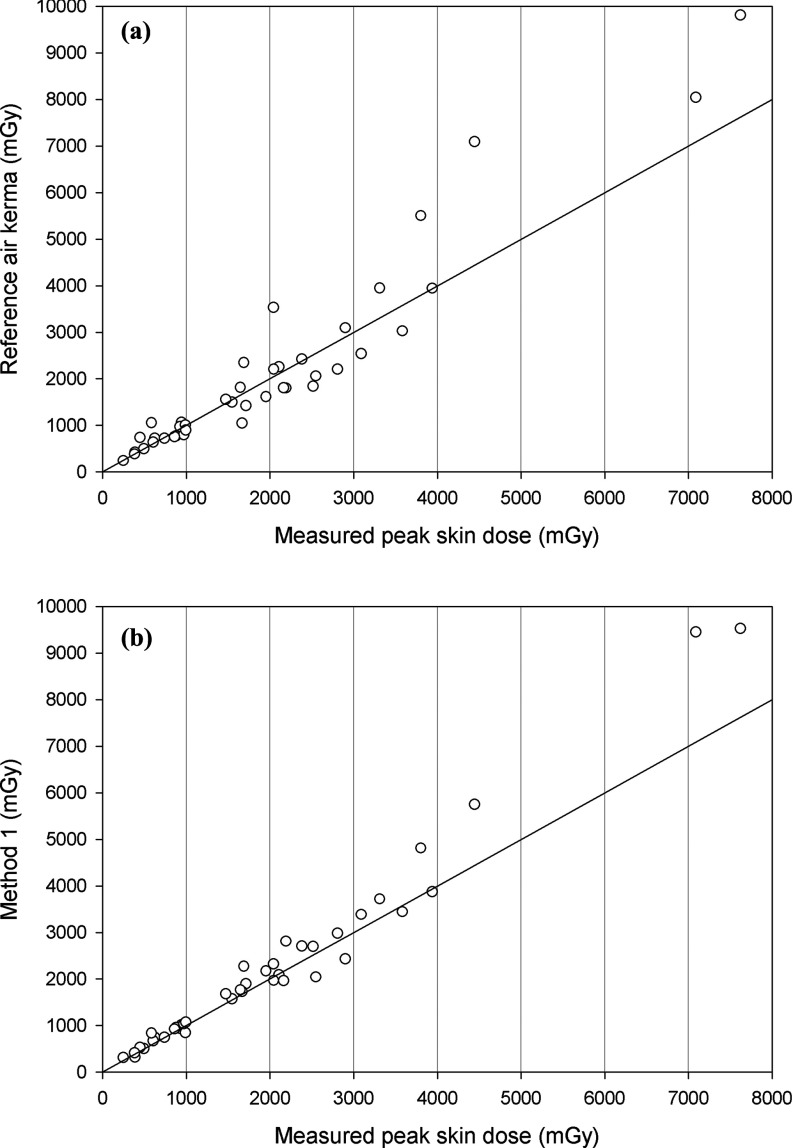
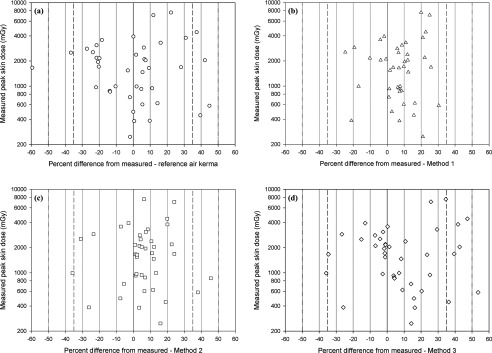
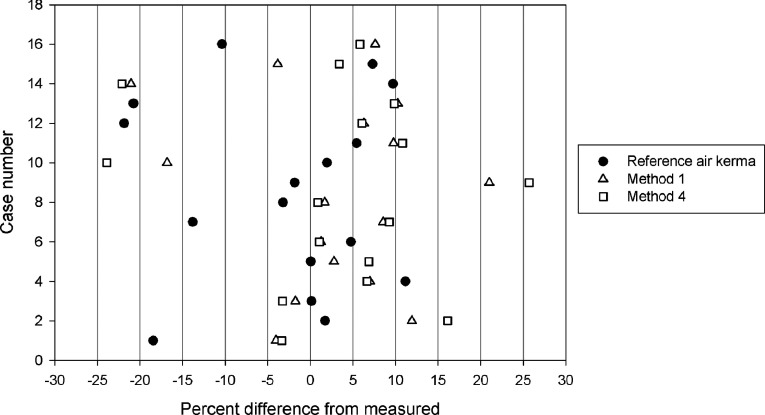
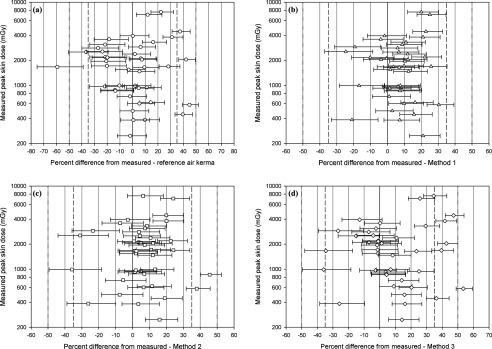
Methods: PSD were measured directly using radiochromic film for 41 consecutive embolization procedures at two sites. Indirect dose metrics from the procedures were collected, including reference air kerma. Four different estimates of PSD were calculated from the indirect dose metrics and compared along with reference air kerma to the measured PSD for each case. The four indirect estimates included a standard calculation method, the use of detailed information from the radiation dose structured report, and two simplified calculation methods based on the standard method. Indirect dosimetry results were compared with direct measurements, including an analysis of uncertainty associated with film dosimetry. Factors affecting the accuracy of the different indirect estimates were examined.
Results: When using the standard calculation method, calculated PSD were within ± 35% for all 41 procedures studied. Calculated PSD were within ± 50% for a simplified method using a single source-to-patient distance for all calculations. Reference air kerma was within ± 50% for all but one procedure. Cases for which reference air kerma or calculated PSD exhibited large (± 35%) differences from the measured PSD were analyzed, and two main causative factors were identified: unusually small or large source-to-patient distances and large contributions to reference air kerma from cone beam computed tomography or acquisition runs acquired at large primary gantry angles. When calculated uncertainty limits [-12.8%, 10%] were applied to directly measured PSD, most indirect PSD estimates remained within ± 50% of the measured PSD.
Conclusions: Using indirect dose metrics, PSD can be determined within ± 35% for embolization procedures. Reference air kerma can be used without modification to set notification limits and substantial radiation dose levels, provided the displayed reference air kerma is accurate. These results can reasonably be extended to similar procedures, including vascular and interventional oncology. Considering these results, film dosimetry is likely an unnecessary effort for these types of procedures when indirect dose metrics are available.
Figures
References
-
- National Cancer Institute, Cancer Therapy Evaluation Program (available URL: http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm). Last accessed April 2014.
-
- Panuccio G., Greenberg R. K., Wunderle K., Mastracci T. M., Eagleton M. G., and Davros W., “Comparison of indirect radiation dose estimates with directly measured radiation dose for patients and operators during complex endovascular procedures,” J. Vasc. Surg. 53, 885–894 (2011).10.1016/j.jvs.2010.10.106 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
