

Antipsychotic polypharmacy in children and adolescents at discharge from psychiatric hospitalization
- PMID: 24990538
- PMCID: PMC4165554
- DOI: 10.1002/phar.1453
Antipsychotic polypharmacy in children and adolescents at discharge from psychiatric hospitalization
Abstract
Study objective: Antipsychotic polypharmacy-the use of more than one antipsychotic concomitantly-has increased in children and adolescents and may be associated with increased adverse effects, nonadherence, and greater costs. Thus, we sought to examine the demographic and clinical characteristics of psychiatrically hospitalized children and adolescents who were prescribed antipsychotic polypharmacy and to identify predictors of this prescribing pattern.
Design: Retrospective medical record review.
Setting: The inpatient psychiatric unit of a large, acute care, urban children's hospital.
Patients: One thousand four hundred twenty-seven children and adolescents who were consecutively admitted and discharged between September 2010 and May 2011.
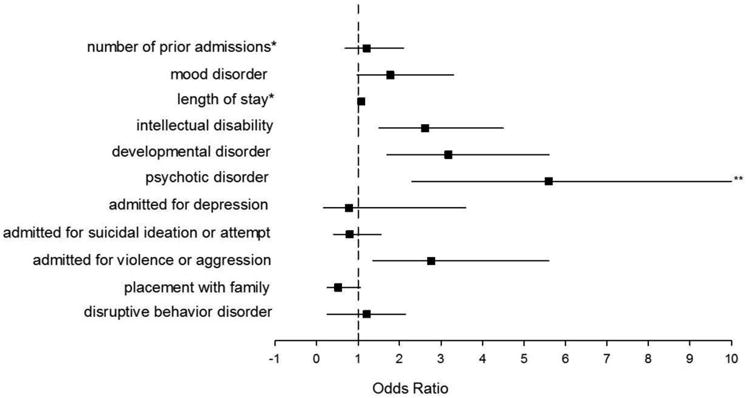
Measurements and main results: At discharge, 840 (58.9%) of the 1427 patients were prescribed one or more antipsychotics, and 99.3% of these received second-generation antipsychotics. Of these 840 patients, 724 (86.2%) were treated with antipsychotic monotherapy, and 116 (13.8%) were treated with antipsychotic polypharmacy. Positive correlations with antipsychotic polypharmacy were observed for placement or custody outside the biological family; a greater number of previous psychiatric admissions; longer hospitalizations; admission for violence/aggression or psychosis; and intellectual disability, psychotic, disruptive behavior, or developmental disorder diagnoses. Negative correlations with antipsychotic polypharmacy included admission for suicidal ideation/attempt or depression, and mood disorder diagnoses. Significant predictors of antipsychotic polypharmacy included admission for violence or aggression (odds ratio [OR] 2.76 [95% confidence interval (CI) 1.36-5.61]), greater number of previous admissions (OR 1.21 [95% CI 1.10-1.33]), and longer hospitalizations (OR 1.08 [95% CI 1.04-1.12]). In addition, diagnoses of intellectual disability (OR 2.62 [95% CI 1.52-4.52]), psychotic disorders (OR 5.60 [95% CI 2.29-13.68]), and developmental disorders (OR 3.18 [95% CI 1.78-5.65]) were predictors of antipsychotic polypharmacy.
Conclusion: Certain youth may have a higher likelihood of being prescribed antipsychotic polypharmacy, which should prompt careful consideration of medication treatment options during inpatient hospitalization. Future examinations of the rationale for combining antipsychotics, along with the long-term safety, tolerability, and cost effectiveness of these therapies, in youth are urgently needed.
Keywords: antipsychotic; child and adolescent psychiatry; polypharmacy; psychiatric hospitalization.
© 2014 Pharmacotherapy Publications, Inc.
Conflict of interest statement
Dr. Saldaña, Ms. Wehry, and Mr. Blom report no biomedical conflicts of interest.
Figures
Similar articles
-
Incident users of antipsychotics: who are they and how do they fare?Soc Psychiatry Psychiatr Epidemiol. 2016 Apr;51(4):505-12. doi: 10.1007/s00127-015-1129-8. Epub 2015 Sep 26. Soc Psychiatry Psychiatr Epidemiol. 2016. PMID: 26409887
-
Prevalence and Factors Affecting the Use of Antipsychotics and Antipsychotic Polypharmacy in a Child and Adolescent Psychiatry Inpatient Service.J Child Adolesc Psychopharmacol. 2023 Mar;33(2):69-75. doi: 10.1089/cap.2022.0065. J Child Adolesc Psychopharmacol. 2023. PMID: 36944095
-
Development and delivery of a quality improvement program to reduce antipsychotic polytherapy.J Manag Care Pharm. 2010 Jul-Aug;16(6):393-401. doi: 10.18553/jmcp.2010.16.6.393. J Manag Care Pharm. 2010. PMID: 20635830 Free PMC article.
-
Prevalence and correlates of antipsychotic polypharmacy in children and adolescents receiving antipsychotic treatment.Int J Neuropsychopharmacol. 2014 Jul;17(7):1095-105. doi: 10.1017/S1461145712001320. Epub 2013 May 14. Int J Neuropsychopharmacol. 2014. PMID: 23673334 Free PMC article. Review.
-
Antipsychotic Polypharmacy Among Patients With Schizophrenia in Africa: A Systematic Review and Meta-Analysis.Int J Neuropsychopharmacol. 2021 Dec 8;24(12):956-964. doi: 10.1093/ijnp/pyab046. Int J Neuropsychopharmacol. 2021. PMID: 34245271 Free PMC article.
Cited by
-
Predictors and Correlates of Psychiatric Polypharmacy Among Child and Adolescent Psychiatric Inpatients: A Retrospective Study.J Clin Psychopharmacol. 2025 May-Jun 01;45(3):243-250. doi: 10.1097/JCP.0000000000001981. Epub 2025 Mar 26. J Clin Psychopharmacol. 2025. PMID: 40132107
-
We Really Need Clear Guidelines and Recommendations for Safer and Proper Use of Aripiprazole and Risperidone in a Pediatric Population: Real-World Analysis of EudraVigilance Database.Front Psychiatry. 2020 Dec 2;11:550201. doi: 10.3389/fpsyt.2020.550201. eCollection 2020. Front Psychiatry. 2020. PMID: 33343407 Free PMC article.
-
Trends Over Time in Antipsychotic Initiation at a Large Children's Health Care System.J Child Adolesc Psychopharmacol. 2021 Jun;31(5):381-386. doi: 10.1089/cap.2020.0190. J Child Adolesc Psychopharmacol. 2021. PMID: 34143677 Free PMC article.
-
A Survey Study on Clinicians' Rationale and Attitude Towards the Prescription of Antipsychotic Polypharmacy in the East Perth Metropolitan Area in Western Australia.Cureus. 2023 Apr 7;15(4):e37234. doi: 10.7759/cureus.37234. eCollection 2023 Apr. Cureus. 2023. PMID: 37064723 Free PMC article.
-
A transdisciplinary team approach to scoping reviews: the case of pediatric polypharmacy.BMC Med Res Methodol. 2018 Oct 4;18(1):102. doi: 10.1186/s12874-018-0560-4. BMC Med Res Methodol. 2018. PMID: 30286720 Free PMC article.
References
-
- Blader JC. Acute inpatient care for psychiatric disorders in the United States, 1996 through 2007. Arch Gen Psychiatry. 2011 Dec;68(12):1276–1283. - PubMed
-
- Olfson M, Blanco C, Liu SM, et al. National trends in the office-based treatment of children, adolescents, and adults with antipsychotics. Arch Gen Psychiatry. 2012 Dec 1;69(12):1247–1256. - PubMed
-
- Olfson M, Crystal S, Huang C, et al. Trends in antipsychotic drug use by very young, privately insured children. J Am Acad Child Adolesc Psychiatry. 2010 Jan;49(1):13–23. - PubMed
-
- Patel NC, Crismon ML, Hoagwood K, et al. Trends in the use of typical and atypical antipsychotics in children and adolescents. J Am Acad Child Adolesc Psychiatry. 2005 Jun;44(6):548–556. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
