

Budget impact model: epigenetic assay can help avoid unnecessary repeated prostate biopsies and reduce healthcare spending
- PMID: 24991343
- PMCID: PMC4031702
Budget impact model: epigenetic assay can help avoid unnecessary repeated prostate biopsies and reduce healthcare spending
Abstract
Background: The diagnosis of prostate cancer involves invasive, sometimes harmful, procedures that can entail negative quality-of-life implications to individuals and high additional costs to the US healthcare system when these procedures result in retesting and iatrogenic harms. It is estimated that $1.86 billion is spent annually on prostate-specific antigen (PSA) testing alone. An advanced epigenetic molecular diagnostic test that uses methylation-specific polymerase chain reaction to assess the DNA methylation status of GSTP1, APC, and RASSF1 genes associated with oncogenesis enables a higher degree of accuracy (previously unattainable through prostate biopsy procedures alone) and produces clinical, financial, and health benefits by reducing the number of medically unnecessary and costly repeated biopsies that are part of today's standard of care.
Objectives: The purpose of this study is to quantify, using a budget impact model, the effect of a relatively new epigenetic assay on healthcare costs for commercial health plans that reimburse for the assay, by avoiding unnecessary repeated prostate biopsy procedures.
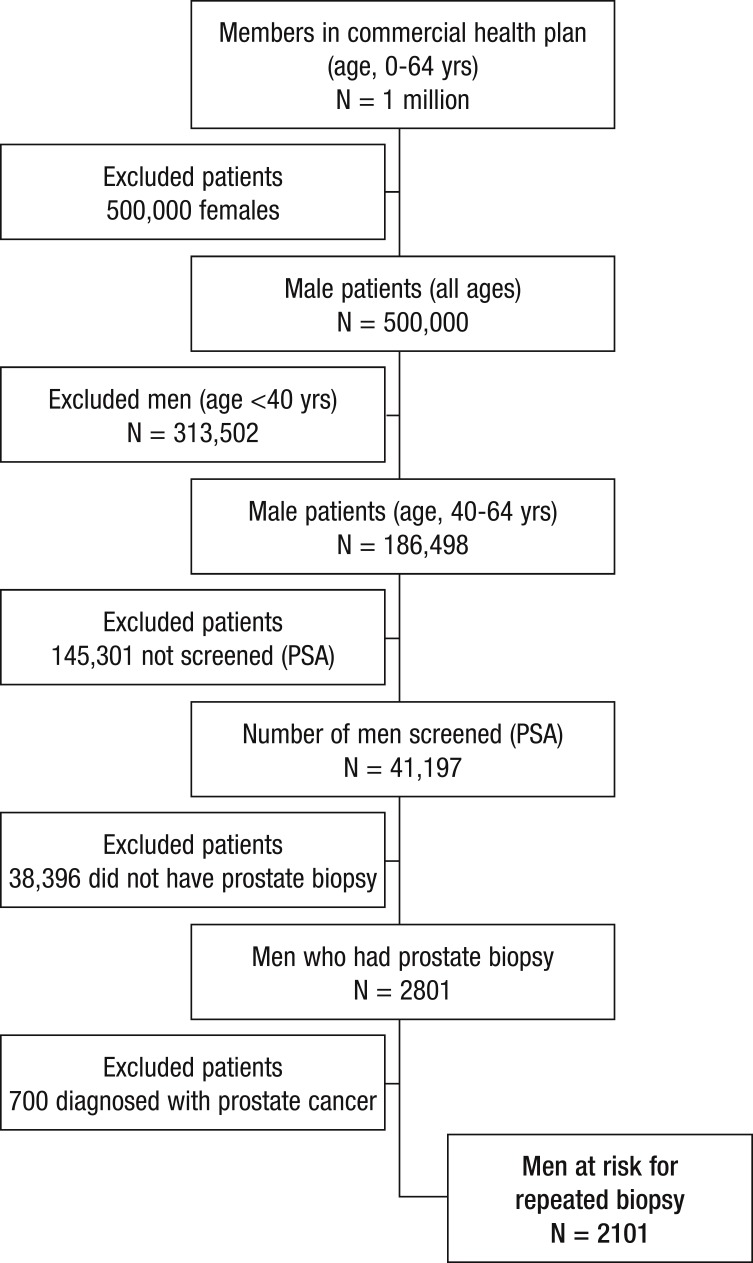
Methods: A budget impact model was developed to test the hypothesis that the epigenetic assay can produce cost-saving benefits to health plans, as well as clinical benefits to urologists and patients with prostate cancer, by providing guidance on how to offer patients more appropriate, and less costly, care. The budget impact model is presented from the perspective of a hypothetical commercial health plan, and direct costs are calculated over a 1-year time horizon, using 2013 Medicare fee-for-service rates. Using a plan of 1 million members, the model compares 1-year costs in a "reference scenario," in which the epigenetic assay is not used for the screening and diagnosis of prostate cancer, to costs in a "new scenario," in which the epigenetic assay is used to distinguish true-negative prostate biopsy results from false-negative biopsy results.
Results: Based on this analysis, administering the epigenetic assay to patients with histopathologically negative biopsies would result in a reduction of 1106 unnecessary biopsies for a health plan with 1 million members. The total 1-year cost of repeated prostate cancer biopsies to the health plan was found to be $2,864,142 in the reference scenario and $2,333,341 in the new scenario. This translates to a total budget impact, or an annual savings, of $530,801 to the plan. The total diagnostic cost was calculated to be $2584 per patient in the new scenario (using the genetic assay) compared with $3172 per patient in the reference scenario (that did not use the assay), resulting in a savings of $588 per patient management.
Conclusion: This analysis shows that the net cost to a commercial health plan with 1 million members would be reduced by approximately $500,000 if patients with histopathologically negative biopsies were managed with the use of the epigenetic assay to differentiate patients who should undergo repeated biopsy and those who should not. Using this genetic-based assay can save costs to health plans and to the US healthcare and improve the clinical management of patients with elevated PSA levels.
Figures
References
-
- Van Neste L, Herman JG, Otto G, et al. The epigenetic promise for prostate cancer diagnosis. Prostate. 2012; 72: 1248–1261 - PubMed
-
- National Cancer Institute. Surveillance, Epidemiology and End Results. 2012. http://seer.cancer.gov/csr/1975_2009_pops09/results_single/sect_01_table... Accessed November 1, 2012.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous