

Resource utilization and cost in a commercially insured population with schizophrenia
- PMID: 24991388
- PMCID: PMC4031739
Resource utilization and cost in a commercially insured population with schizophrenia
Abstract
Background: Schizophrenia is a serious public health concern and a leading cause of disability. Previous studies have shown this disease is associated with an economic burden of more than $60 billion annually in direct and indirect costs in the United States.
Objective: To analyze the annual and longitudinal costs associated with the treatment of patients with schizophrenia from a payer perspective.
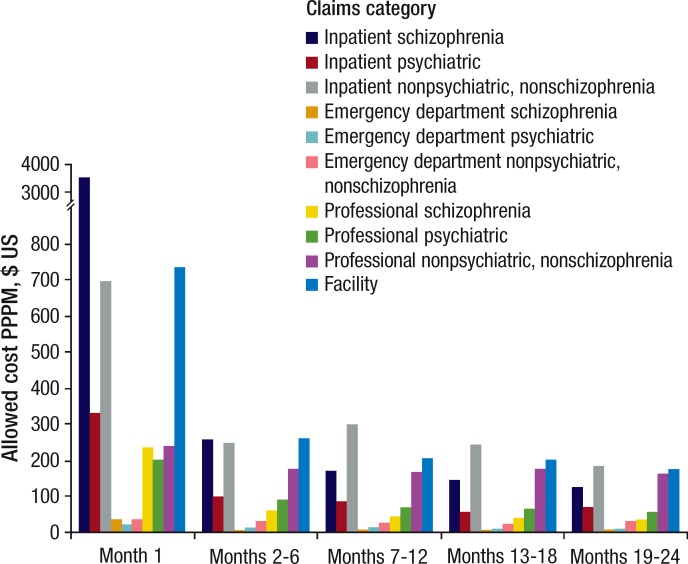
Methods: Two claim-based analyses were conducted using data from the Truven Health MarketScan database of a commercially insured population: (1) an annual snapshot of patients with newly diagnosed and chronic schizophrenia, and (2) a 24-month longitudinal analysis of patients with newly diagnosed schizophrenia. The snapshot analysis included individuals who had ≥2 claims with a diagnosis code for schizophrenia on separate dates during 2011 (with the date of the first claim designated as the index date), and who were enrolled for 12 months before the index date. For the longitudinal analysis, patients were included if they were continuously enrolled for 24 months after the date of schizophrenia diagnosis, which was designated as the index date. The claims were grouped by inpatient, outpatient, professional, and prescription drug categories, and were further segmented by claims for schizophrenia, other psychiatric, and nonschizophrenia/nonpsychiatric conditions.
Results: A total of 8985 patients with schizophrenia met the inclusion criteria for the snapshot analysis. The mean cost per patient per month (PPPM) for a patient with schizophrenia was $1806 versus $419 per member per month for the demographically adjusted nonschizophrenic (ie, matched for age and sex) population. The PPPM cost of $1806 for patients with schizophrenia was 42% for inpatient expenditures, 33% for outpatient, and 25% for prescription drug costs. The annual inpatient admission rates were 636 per 1000 patients with schizophrenia and 48 per 1000 persons for the demographically adjusted population without schizophrenia. The annual emergency department visits for patients with schizophrenia were 2270 per 1000 patients and 158 per 1000 persons without schizophrenia for the demographically adjusted population. For the longitudinal analysis, 1902 patients with newly diagnosed schizophrenia were identified. The total claim costs for patients increased from $800 monthly in the 12 months before the index date to approximately $2000 in the month before the index date. The highest costs occurred in the month of diagnosis (designated as the index month; mean cost, $6601). The total all-cause claim cost after the index date decreased to $1635 monthly for months 2 to 6, $1456 monthly for months 7 to 12, $1324 monthly for months 13 to 18, and $1218 monthly for months 19 to 24.
Conclusion: Although the prevalence of schizophrenia is low in a commercially insured US population, this analysis shows that the average total claim cost per patient with schizophrenia is more than 4 times the average total claim cost for a demographically adjusted population without schizophrenia. Furthermore, for newly diagnosed patients with schizophrenia, the cost, which is largely driven by inpatient charges, is highest in the month of diagnosis.
Figures



Similar articles
-
Economic Burden of Irritable Bowel Syndrome with Diarrhea: Retrospective Analysis of a U.S. Commercially Insured Population.J Manag Care Spec Pharm. 2017 Apr;23(4):453-460. doi: 10.18553/jmcp.2016.16138. Epub 2016 Nov 21. J Manag Care Spec Pharm. 2017. PMID: 28345443 Free PMC article.
-
Disease-related and all-cause health care costs of elderly patients with gout.J Manag Care Pharm. 2008 Mar;14(2):164-75. doi: 10.18553/jmcp.2008.14.2.164. J Manag Care Pharm. 2008. PMID: 18331118 Free PMC article.
-
Actuarial analysis of private payer administrative claims data for women with endometriosis.J Manag Care Pharm. 2007 Apr;13(3):262-72. doi: 10.18553/jmcp.2007.13.3.262. J Manag Care Pharm. 2007. PMID: 17407392 Free PMC article.
-
Health Care Resource Utilization and Cost Before Initial Schizophrenia Diagnosis.J Manag Care Spec Pharm. 2019 Oct;25(10):1102-1110. doi: 10.18553/jmcp.2019.25.10.1102. J Manag Care Spec Pharm. 2019. PMID: 31556820 Free PMC article.
-
[Cost-effectiveness analysis of schizophrenic patient care settings: impact of an atypical antipsychotic under long-acting injection formulation].Encephale. 2005 Mar-Apr;31(2):235-46. doi: 10.1016/s0013-7006(05)82390-5. Encephale. 2005. PMID: 15959450 Review. French.
Cited by
-
Pharmaco-utilisation and related costs of drugs used to treat schizophrenia and bipolar disorder in Italy: the IBIS study.BMC Psychiatry. 2014 Oct 14;14:282. doi: 10.1186/s12888-014-0282-z. BMC Psychiatry. 2014. PMID: 25312446 Free PMC article. Clinical Trial.
-
Healthcare utilization among patients with psychiatric hospitalization admitted through the emergency department (ED): A claims-based study.Gen Hosp Psychiatry. 2020 Nov-Dec;67:92-99. doi: 10.1016/j.genhosppsych.2020.10.001. Epub 2020 Oct 7. Gen Hosp Psychiatry. 2020. PMID: 33068850 Free PMC article.
-
Economic Burden of Treatment-Resistant Depression on the U.S. Health Care System.J Manag Care Spec Pharm. 2019 Jul;25(7):823-835. doi: 10.18553/jmcp.2019.25.7.823. J Manag Care Spec Pharm. 2019. PMID: 31232205 Free PMC article.
-
Adherence and rehospitalizations in patients with schizophrenia: evidence from Japanese claims data.Neuropsychiatr Dis Treat. 2015 Apr 1;11:935-40. doi: 10.2147/NDT.S81677. eCollection 2015. Neuropsychiatr Dis Treat. 2015. PMID: 25897229 Free PMC article.
-
Patient Journey of Veterans with Schizophrenia: An Analysis of Treatment Patterns, Healthcare Resource Utilization and Costs.Adv Ther. 2022 Mar;39(3):1199-1214. doi: 10.1007/s12325-021-01997-z. Epub 2022 Jan 7. Adv Ther. 2022. PMID: 34994955
References
-
- Regier DA, Narrow WE, Rae DS, et al. The de facto US mental and addictive disorders service system. Epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry. 1993; 50: 85–94 - PubMed
-
- Wu EQ, Birnbaum HG, Shi L, et al. The economic burden of schizophrenia in the United States in 2002. J Clin Psychiatry. 2005; 66: 1122–1129 - PubMed
-
- World Health Organization. Schizophrenia. www.who.int/mental_health/management/schizophrenia/en/ Accessed September 26, 2013.
LinkOut - more resources
Full Text Sources
Miscellaneous