

Acute hemodynamic effects of riociguat in patients with pulmonary hypertension associated with diastolic heart failure (DILATE-1): a randomized, double-blind, placebo-controlled, single-dose study
- PMID: 24991733
- PMCID: PMC4219342
- DOI: 10.1378/chest.14-0106
Acute hemodynamic effects of riociguat in patients with pulmonary hypertension associated with diastolic heart failure (DILATE-1): a randomized, double-blind, placebo-controlled, single-dose study
Abstract
Background: Deficient nitric oxide-soluble guanylate cyclase-cyclic guanosine monophosphate signaling results from endothelial dysfunction and may underlie impaired cardiac relaxation in patients with heart failure with preserved left ventricular ejection fraction (HFpEF) and pulmonary hypertension (PH). The acute hemodynamic effects of riociguat, a novel soluble guanylate cyclase stimulator, were characterized in patients with PH and HFpEF.
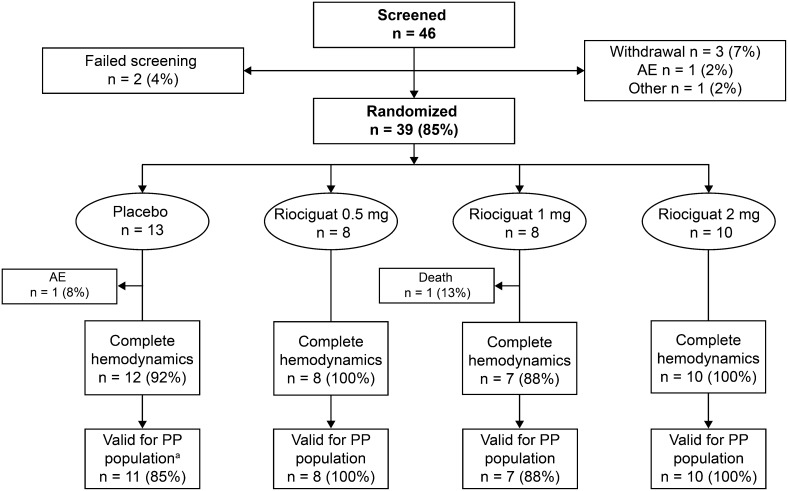
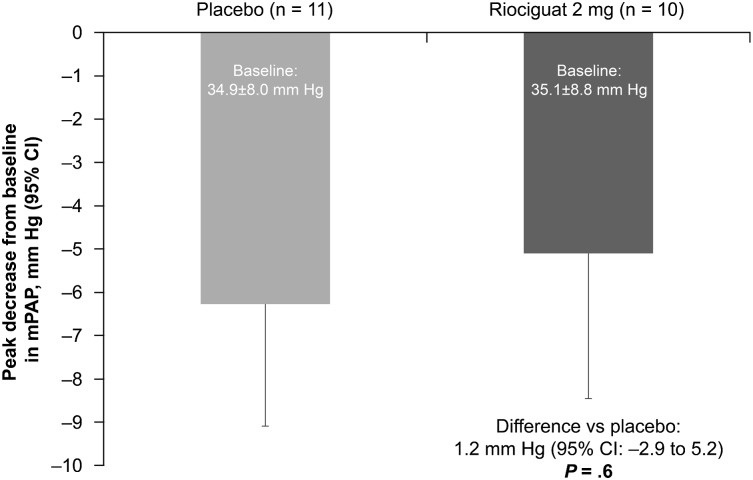
Methods: Clinically stable patients receiving standard HF therapy with a left ventricular ejection fraction > 50%, mean pulmonary artery pressure (mPAP) ≥ 25 mm Hg, and pulmonary arterial wedge pressure (PAWP) > 15 mm Hg at rest were randomized to single oral doses of placebo or riociguat (0.5, 1, or 2 mg). The primary efficacy variable was the peak decrease in mPAP from baseline up to 6 h. Secondary outcomes included hemodynamic and echocardiographic parameters, safety, and pharmacokinetics.
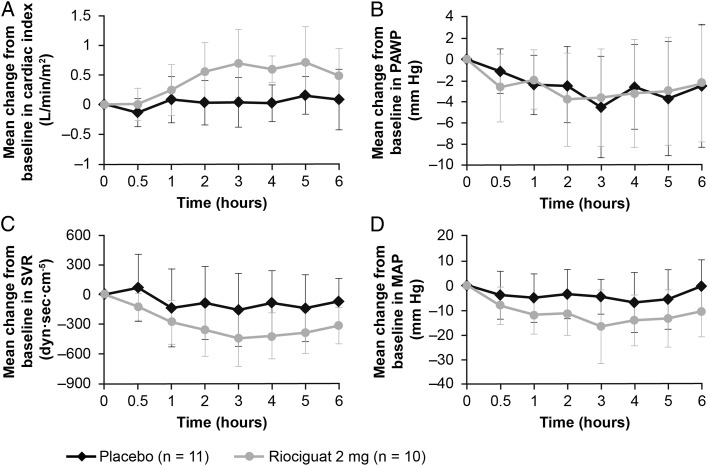
Results: There was no significant change in peak decrease in mPAP with riociguat 2 mg (n = 10) vs placebo (n = 11, P = .6). However, riociguat 2 mg significantly increased stroke volume (+9 mL [95% CI, 0.4-17]; P = .04) and decreased systolic BP (-12 mm Hg [95% CI, -22 to -1]; P = .03) and right ventricular end-diastolic area (-5.6 cm2 [95% CI, -11 to -0.3]; P = .04), without significantly changing heart rate, PAWP, transpulmonary pressure gradient, or pulmonary vascular resistance. Riociguat was well tolerated.
Conclusions: In patients with HFpEF and PH, riociguat was well tolerated, had no significant effect on mPAP, and improved exploratory hemodynamic and echocardiographic parameters.
Trial registry: ClinicalTrials.gov; No.: NCT01172756; URL: www.clinicaltrials.gov.
Figures
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355(3):251-259 - PubMed
-
- McMurray JJ, Adamopoulos S, Anker SD, et al. ; ESC Committee for Practice Guidelines. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33(14):1787-1847 - PubMed
-
- Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure—abnormalities in active relaxation and passive stiffness of the left ventricle. N Engl J Med. 2004;350(19):1953-1959 - PubMed
-
- Kawaguchi M, Hay I, Fetics B, Kass DA. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: implications for systolic and diastolic reserve limitations. Circulation. 2003;107(5):714-720 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
