

An individual patient data meta-analysis on characteristics and outcome of patients with papillary glioneuronal tumor, rosette glioneuronal tumor with neuropil-like islands and rosette forming glioneuronal tumor of the fourth ventricle
- PMID: 24991807
- PMCID: PMC4084640
- DOI: 10.1371/journal.pone.0101211
An individual patient data meta-analysis on characteristics and outcome of patients with papillary glioneuronal tumor, rosette glioneuronal tumor with neuropil-like islands and rosette forming glioneuronal tumor of the fourth ventricle
Abstract
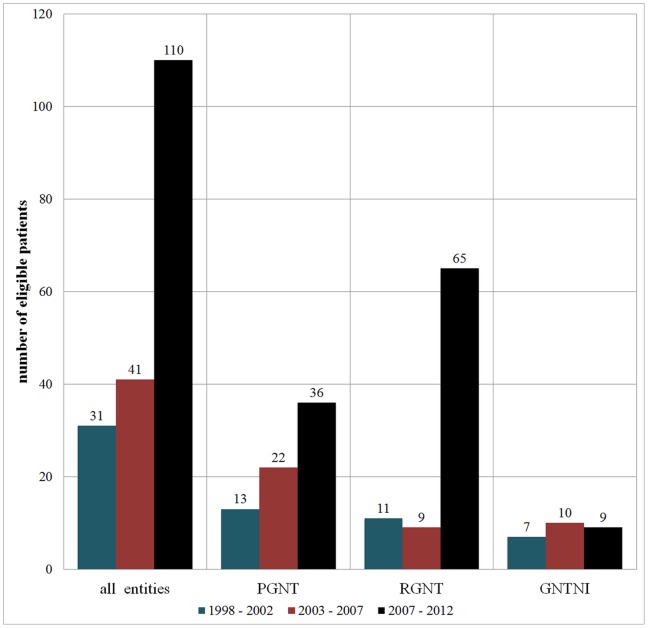
Background and purpose: In 2007, the WHO classification of brain tumors was extended by three new entities of glioneuronal tumors: papillary glioneuronal tumor (PGNT), rosette-forming glioneuronal tumor of the fourth ventricle (RGNT) and glioneuronal tumor with neuropil-like islands (GNTNI). Focusing on clinical characteristics and outcome, the authors performed a comprehensive individual patient data (IPD) meta-analysis of the cases reported in literature until December 2012.
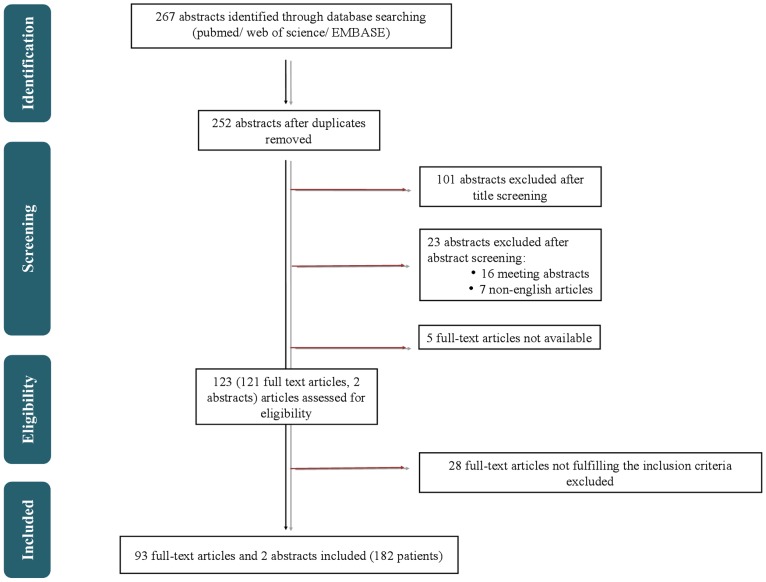
Methods: PubMed, Embase and Web of Science were searched for peer-reviewed articles reporting on PGNT, RGNT, and GNTNI using predefined keywords.
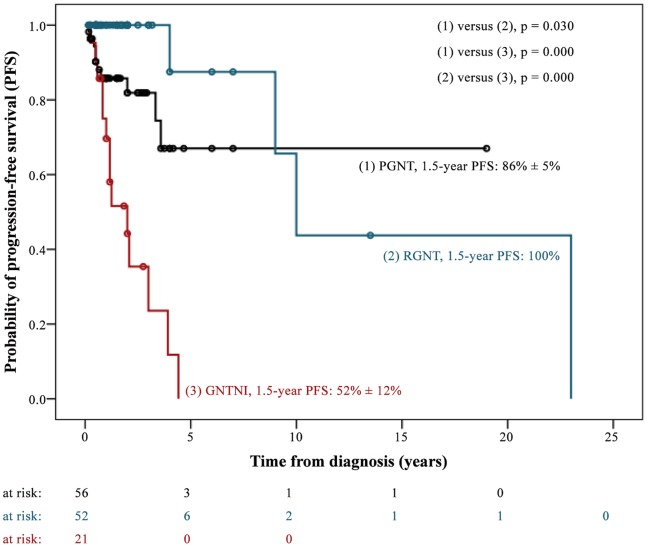
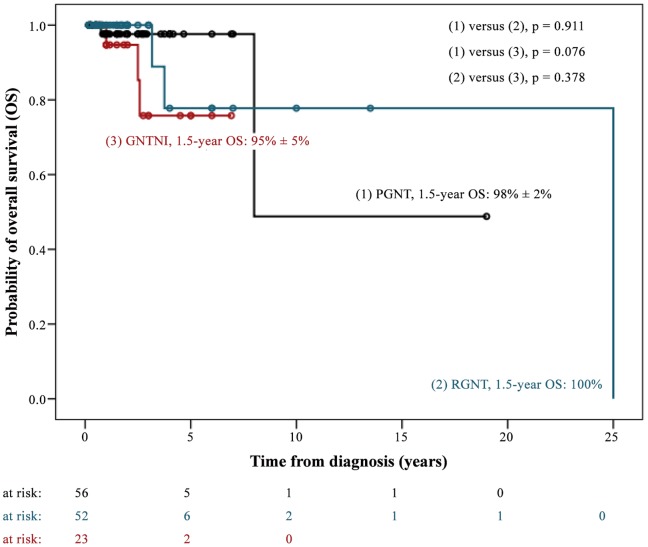
Results: 95 publications reported on 182 patients (PGNT, 71; GNTNI, 26; RGNT, 85). Median age at diagnosis was 23 years (range 4-75) for PGNT, 27 years (range 6-79) for RGNT, and 40 years (range 2-65) for GNTNI. Ninety-seven percent of PGNT and 69% of GNTNI were located in the supratentorial region, 23% of GNTNI were in the spinal cord, and 80% of RGNT were localized in the posterior fossa. Complete resection was reported in 52 PGNT (73%), 36 RGNT (42%), and 7 GNTNI (27%) patients. Eight PGNT, 3 RGNT, and 12 GNTNI patients were treated with chemo- and/or radiotherapy as the primary postoperative treatment. Follow-up data were available for 132 cases. After a median follow-up time of 1.5 years (range 0.2-25) across all patients, 1.5-year progression-free survival rates were 52±12% for GNTNI, 86±5% for PGNT, and 100% for RGNT. The 1.5-year overall-survival were 95±5%, 98±2%, and 100%, respectively.
Conclusions: The clinical understanding of the three new entities of glioneuronal tumors, PGNT, RGNT and GNTNI, is currently emerging. The present meta-analysis will hopefully contribute to a delineation of their diagnostic, therapeutic, and prognostic profiles. However, the available data do not provide a solid basis to define the optimum treatment approach. Hence, a central register should be established.
Conflict of interest statement
Figures
References
-
- Adachi J, Nishikawa R, Hirose T, Matsutani M (2005) Mixed neuronal-glial tumor of the fourth ventricle and successful treatment of postoperative mutism with bromocriptine: case report. Surg Neurol 63: 375–379. - PubMed
-
- Agarwal S, Sharma MC, Singh G, Suri V, Sarkar C, et al. (2012) Papillary glioneuronal tumor - a rare entity: report of four cases and brief review of literature. Childs Nerv Syst 28: 1897–1904. - PubMed
-
- Allende DS, Prayson RA (2009) The expanding family of glioneuronal tumors. Adv Anat Pathol 16: 33–39. - PubMed
-
- Amemiya S, Shibahara J, Aoki S, Takao H, Ohtomo K (2008) Recently established entities of central nervous system tumors: review of radiological findings. J Comput Assist Tomogr 32: 279–285. - PubMed
-
- Anan M, Inoue R, Ishii K, Abe T, Fujiki M, et al. (2009) A rosette-forming glioneuronal tumor of the spinal cord: the first case of a rosette-forming glioneuronal tumor originating from the spinal cord. Hum Pathol 40: 898–901. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
