

Sleep disordered breathing, fatigue, and sleepiness in HIV-infected and -uninfected men
- PMID: 24991815
- PMCID: PMC4084642
- DOI: 10.1371/journal.pone.0099258
Sleep disordered breathing, fatigue, and sleepiness in HIV-infected and -uninfected men
Abstract
Study objectives: We investigated the association of HIV infection and highly active antiretroviral therapy (HAART) with sleep disordered breathing (SDB), fatigue, and sleepiness.
Methods: HIV-uninfected men (HIV-; n = 60), HIV-infected men using HAART (HIV+/HAART+; n = 58), and HIV-infected men not using HAART (HIV+/HAART-; n = 41) recruited from two sites of the Multicenter AIDS cohort study (MACS) underwent a nocturnal sleep study, anthropometric assessment, and questionnaires for fatigue and the Epworth Sleepiness Scale. The prevalence of SDB in HIV- men was compared to that in men matched from the Sleep Heart Health Study (SHHS).
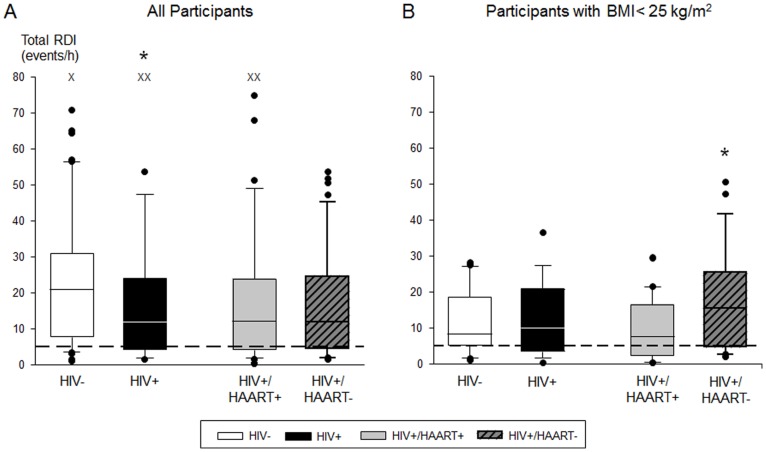
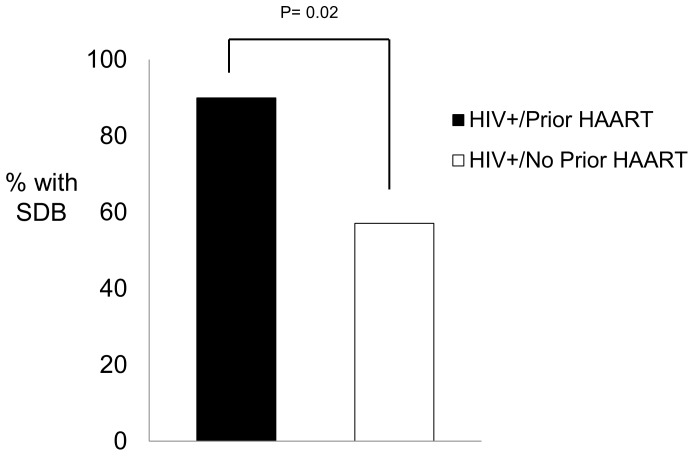
Results: The prevalence of SDB was unexpectedly high in all groups: 86.7% for HIV-, 70.7% for HIV+/HAART+, and 73.2% for HIV+/HAART-, despite lower body-mass indices (BMI) in HIV+ groups. The higher prevalence in the HIV- men was significant in univariate analyses but not after adjustment for BMI and other variables. SDB was significantly more common in HIV- men in this study than those in SHHS, and was common in participants with BMIs <25 kg/m2. HIV+ men reported fatigue more frequently than HIV- men (25.5% vs. 6.7%; p = 0.003), but self-reported sleepiness did not differ among the three groups. Sleepiness, but not fatigue, was significantly associated with SDB.
Conclusions: SDB was highly prevalent in HIV- and HIV+ men, despite a normal or slightly elevated BMI. The high rate of SDB in men who have sex with men deserves further investigation. Sleepiness, but not fatigue, was related to the presence of SDB. Clinicians caring for HIV-infected patients should distinguish between fatigue and sleepiness when considering those at risk for SDB, especially in non-obese men.
Conflict of interest statement
Figures
References
-
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, et al. (1993) The occurrence of sleep-disordered breathing among middle-aged adults. NEnglJ Med 328: 1230–1235. - PubMed
-
- Punjabi NM, O’Hearn DJ, Neubauer DN, Nieto FJ, Schwartz AR, et al. (1999) Modeling hypersomnolence in sleep-disordered breathing. A novel approach using survival analysis. AmJ Respir Crit Care Med 159: 1703–1709. - PubMed
-
- Adams N, Strauss M, Schluchter M, Redline S (2001) Relation of measures of sleep-disordered breathing to neuropsychological functioning. Am J Respir Crit Care Med 163: 1626–1631. - PubMed
-
- Chervin RD (2000) Sleepiness, fatigue, tiredness, and lack of energy in obstructive sleep apnea. Chest 118: 372–379. - PubMed
-
- Aguillard RN, Riedel BW, Lichstein KL, Grieve FG, Johnson CT, et al. (1998) Daytime functioning in obstructive sleep apnea patients: exercise tolerance, subjective fatigue, and sleepiness. Appl PsychophysiolBiofeedback 23: 207–217. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 AI035042/AI/NIAID NIH HHS/United States
- U01-AI-35042/AI/NIAID NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- K23 HL077137/HL/NHLBI NIH HHS/United States
- R01-HL07955/HL/NHLBI NIH HHS/United States
- U01-AI-35041/AI/NIAID NIH HHS/United States
- K23-AT2862/AT/NCCIH NIH HHS/United States
- U01 AI035041/AI/NIAID NIH HHS/United States
- UM1 AI035043/AI/NIAID NIH HHS/United States
- U01 AI035043/AI/NIAID NIH HHS/United States
- U01-AI-35043/AI/NIAID NIH HHS/United States
- U01HL53937/HL/NHLBI NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- UL1-RR-025005/RR/NCRR NIH HHS/United States
- U01 HL053937/HL/NHLBI NIH HHS/United States
- K23-HL77137/HL/NHLBI NIH HHS/United States
- T32 HL007955/HL/NHLBI NIH HHS/United States
- K23 AT002862/AT/NCCIH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
