

Temporal changes in the outcomes of HIV-exposed infants in Kinshasa, Democratic Republic of Congo during a period of rapidly evolving guidelines for care (2007-2013)
- PMID: 24991903
- PMCID: PMC4600322
- DOI: 10.1097/QAD.0000000000000331
Temporal changes in the outcomes of HIV-exposed infants in Kinshasa, Democratic Republic of Congo during a period of rapidly evolving guidelines for care (2007-2013)
Abstract
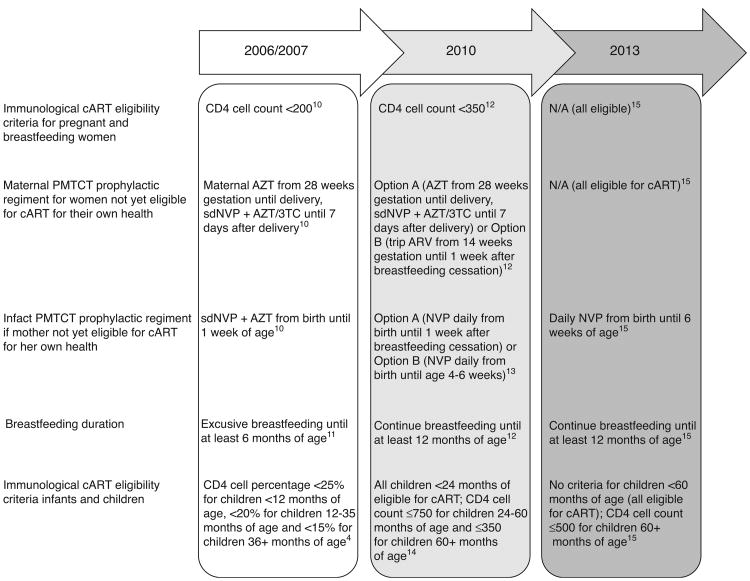
Objective: Guidelines for prevention of mother-to-child transmission of HIV have developed rapidly, yet little is known about how outcomes of HIV-exposed infants have changed over time. We describe HIV-exposed infant outcomes in Kinshasa, Democratic Republic of Congo, between 2007 and 2013.
Design: Cohort study of mother-infant pairs enrolled in family-centered comprehensive HIV care.
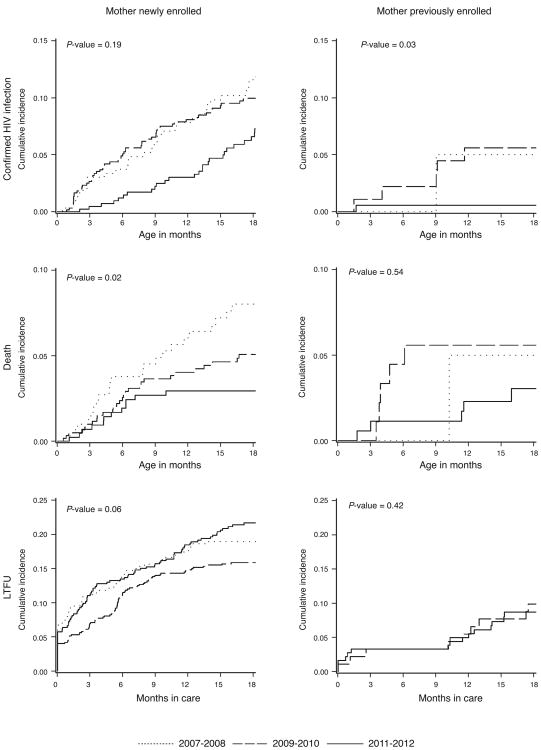
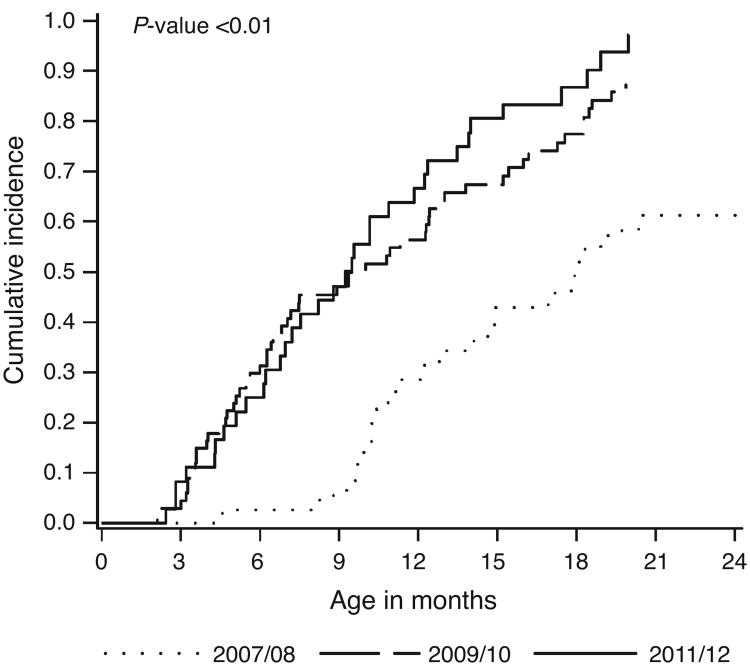
Methods: Accounting for competing risks, we estimated the cumulative incidences of early infant diagnosis, HIV transmission, death, loss to follow-up, and combination antiretroviral therapy (cART) initiation for infants enrolled in three periods (2007-2008, 2009-2010, and 2011-2012).
Results: 1707 HIV-exposed infants enrolled at a median age of 2.6 weeks. Among infants whose mothers had recently enrolled into HIV care (N = 1411), access to EID by age two months increased from 28% (95% confidence limits [CL]: 24,34%) among infants enrolled in 2007-2008 to 63% (95% CL: 59,68%) among infants enrolled in 2011-2012 (Gray's p-value <0.01). The 18-month cumulative incidence of HIV declined from 16% (95% CL: 11,22%) for infants enrolled in 2007-2008 to 11% (95% CL: 8,16%) for infants enrolled in 2011-2012 (Gray's p-value = 0.19). The 18-month cumulative incidence of death also declined, from 8% (95% CL: 5,12%) to 3% (95% CL: 2,5%) (Gray's p-value = 0.02). LTFU did not improve, with 18-month cumulative incidences of 19% (95% CL: 15,23%) for infants enrolled in 2007-2008 and 22% (95% CL: 18,26%) for infants enrolled in 2011-2012 (Gray's p-value = 0.06). Among HIV-infected infants, the 24-month cumulative incidence of cART increased from 61% (95% CL: 43,75%) to 97% (95% CL: 82,100%) (Gray's p-value <0.01); the median age at cART decreased from 17.9 to 9.3 months. Outcomes were better for infants whose mothers enrolled before pregnancy.
Conclusions: We observed encouraging improvements, but continued efforts are needed.
Conflict of interest statement
Figures
Similar articles
-
Implementation and Operational Research: Decentralization Does Not Assure Optimal Delivery of PMTCT and HIV-Exposed Infant Services in a Low Prevalence Setting.J Acquir Immune Defic Syndr. 2015 Dec 1;70(4):e130-9. doi: 10.1097/QAI.0000000000000781. J Acquir Immune Defic Syndr. 2015. PMID: 26262776 Free PMC article.
-
Implementation and Operational Research: Maternal Combination Antiretroviral Therapy Is Associated With Improved Retention of HIV-Exposed Infants in Kinshasa, Democratic Republic of Congo.J Acquir Immune Defic Syndr. 2015 Jul 1;69(3):e93-9. doi: 10.1097/QAI.0000000000000644. J Acquir Immune Defic Syndr. 2015. PMID: 25886922 Free PMC article.
-
Rates and Predictors of HIV-Exposed Infants Lost to Follow-Up During Early Infant Diagnosis Services in Kenya.AIDS Patient Care STDS. 2019 Aug;33(8):346-353. doi: 10.1089/apc.2019.0050. AIDS Patient Care STDS. 2019. PMID: 31369296 Free PMC article.
-
Early Antiretroviral Therapy Initiation and Mortality Among Infants Diagnosed With HIV in the First 12 Weeks of Life: Experiences From Kinshasa, DR Congo and Blantyre, Malawi.Pediatr Infect Dis J. 2017 Jul;36(7):654-658. doi: 10.1097/INF.0000000000001539. Pediatr Infect Dis J. 2017. PMID: 28060044 Free PMC article.
-
Improved access to early infant diagnosis is a critical part of a child-centric prevention of mother-to-child transmission agenda.AIDS. 2013 Nov;27 Suppl 2:S197-205. doi: 10.1097/QAD.0000000000000104. AIDS. 2013. PMID: 24361629 Review.
Cited by
-
Implementation and Operational Research: Decentralization Does Not Assure Optimal Delivery of PMTCT and HIV-Exposed Infant Services in a Low Prevalence Setting.J Acquir Immune Defic Syndr. 2015 Dec 1;70(4):e130-9. doi: 10.1097/QAI.0000000000000781. J Acquir Immune Defic Syndr. 2015. PMID: 26262776 Free PMC article.
-
Paediatric HIV: Progress on Prevention, Treatment and Cure.Curr Pediatr Rep. 2015 Sep;3(3):219-229. doi: 10.1007/s40124-015-0087-7. Epub 2015 Jul 22. Curr Pediatr Rep. 2015. PMID: 26709366 Free PMC article.
-
Implementation and Operational Research: Maternal Combination Antiretroviral Therapy Is Associated With Improved Retention of HIV-Exposed Infants in Kinshasa, Democratic Republic of Congo.J Acquir Immune Defic Syndr. 2015 Jul 1;69(3):e93-9. doi: 10.1097/QAI.0000000000000644. J Acquir Immune Defic Syndr. 2015. PMID: 25886922 Free PMC article.
-
High prevalence of impaired glucose metabolism among children and adolescents living with HIV in Ghana.HIV Med. 2024 May;25(5):577-586. doi: 10.1111/hiv.13614. Epub 2024 Jan 19. HIV Med. 2024. PMID: 38240173 Free PMC article.
-
Predictors of Infant Age at Enrollment in Early Infant Diagnosis Services in Kenya.AIDS Behav. 2016 Sep;20(9):2141-50. doi: 10.1007/s10461-016-1404-z. AIDS Behav. 2016. PMID: 27108002 Free PMC article.
References
-
- UNAIDS. Global report: UNAIDS report on the global AIDS epidemic 2013. UNAIDS; 2013.
-
- UNAIDS. Countdown to zero: global plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive (2011 – 2015) UNAIDS; 2011. - PubMed
-
- World Health Organization and UNICEF. Countdown to 2015: maternal, newborn and child survival: building a future for women and children: the 2012 report. World Health Organization; 2012.
-
- World Health Organization. Antiretroviral therapy of HIV infection in infants and children: towards universal access: recommendations for a public health approach (2006) World Health Organization; 2007. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
