

Amniotic membrane grafts for the prevention of esophageal stricture after circumferential endoscopic submucosal dissection
- PMID: 24992335
- PMCID: PMC4081114
- DOI: 10.1371/journal.pone.0100236
Amniotic membrane grafts for the prevention of esophageal stricture after circumferential endoscopic submucosal dissection
Abstract
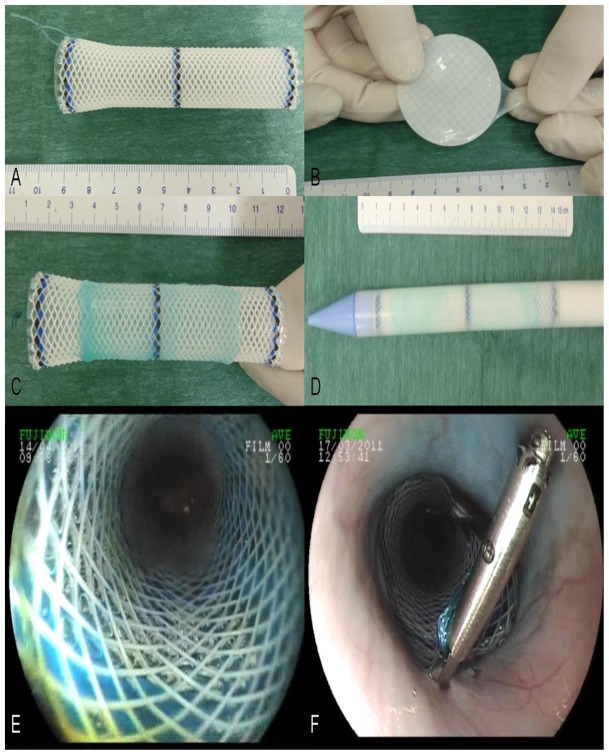
Background and aims: The prevention of esophageal strictures following circumferential mucosal resection remains a major clinical challenge. Human amniotic membrane (AM) is an easily available material, which is widely used in ophthalmology due to its wound healing, anti-inflammatory and anti-fibrotic properties. We studied the effect of AM grafts in the prevention of esophageal stricture after endoscopic submucosal dissection (ESD) in a swine model.
Animals and methods: In this prospective, randomized controlled trial, 20 swine underwent a 5 cm-long circumferential ESD of the lower esophagus. In the AM Group (n = 10), amniotic membrane grafts were placed on esophageal stents; a subgroup of 5 swine (AM 1 group) was sacrificed on day 14, whereas the other 5 animals (AM 2 group) were kept alive. The esophageal stent (ES) group (n = 5) had ES placement alone after ESD. Another 5 animals served as a control group with only ESD.
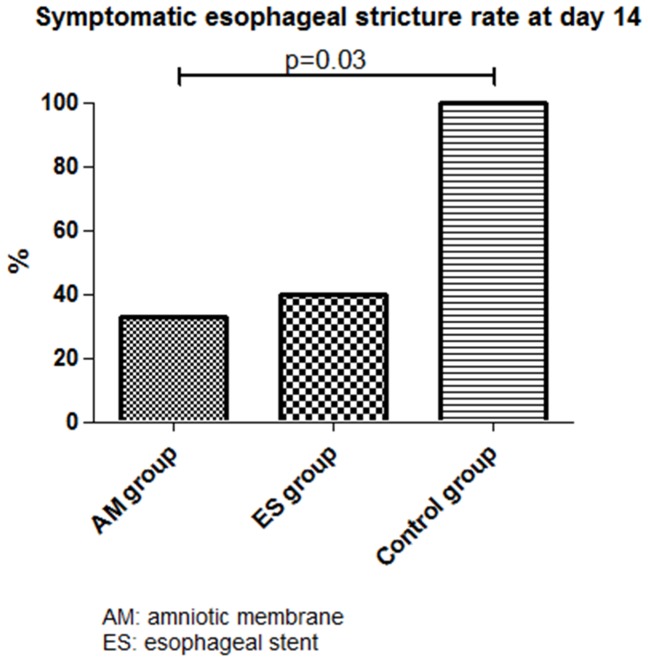
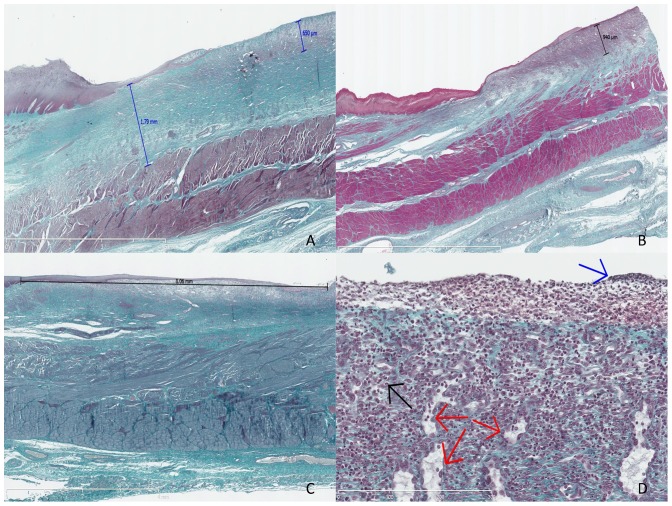
Results: The prevalence of symptomatic strictures at day 14 was significantly reduced in the AM group and ES groups vs. the control group (33%, 40% and 100%, respectively, p = 0.03); mean esophageal diameter was 5.8±3.6 mm, 6.8±3.3 mm, and 2.6±1.7 mm for AM, ES, and control groups, respectively. Median (range) esophageal fibrosis thickness was 0.87 mm (0.78-1.72), 1.19 mm (0.28-1.95), and 1.65 mm (0.7-1.79) for AM 1, ES, and control groups, respectively. All animals had developed esophageal strictures by day 35.
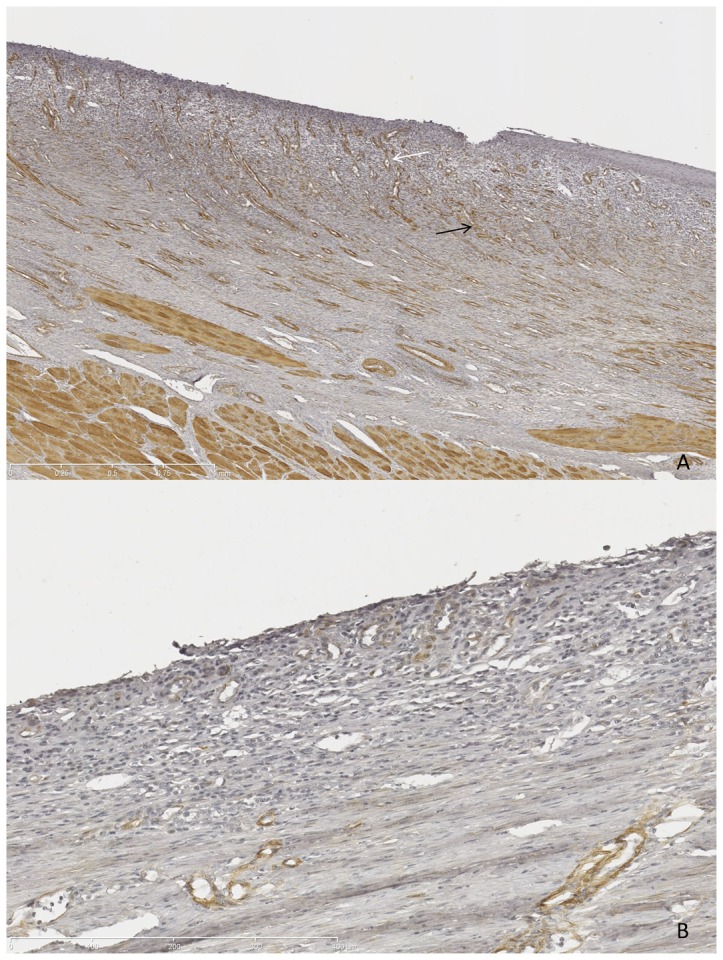
Conclusions: The anti-fibrotic effect of AM on esophageal wound healing after ESD delayed the development of esophageal stricture in our model. However, this benefit was of limited duration in the conditions of our study.
Conflict of interest statement
Figures
References
-
- Shaheen NJ, Richter JE (2009) Barrett's oesophagus. Lancet 373: 850–861. - PubMed
-
- Chennat J, Konda VJ, Ross AS, de Tejada AH, Noffsinger A, et al. (2009) Complete Barrett's eradication endoscopic mucosal resection: an effective treatment modality for high-grade dysplasia and intramucosal carcinoma–an American single-center experience. Am J Gastroenterol 104: 2684–2692. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
