

Use of the surgical Apgar score to guide postoperative care
- PMID: 24992418
- PMCID: PMC4473931
- DOI: 10.1308/003588414X13946184900840
Use of the surgical Apgar score to guide postoperative care
Abstract
Introduction: The surgical Apgar score (SAS) can predict 30-day major complications or death after surgery. Studies have validated the score in different patient populations and suggest it should be used to objectively guide postoperative care. We aimed to see whether using the SAS in a decisive approach in a future randomised controlled trial (RCT) would be likely to demonstrate an effect on postoperative care and clinical outcome.
Methods: A total of 143 adults undergoing general/vascular surgery in 9 National Health Service hospitals were recruited to a pilot single blinded RCT and the data for 139 of these were analysed. Participants were randomised to a control group with standard postoperative care or to an intervention group with care influenced (but not mandated) by the SAS (decisive approach). The notional primary outcome was 30-day major complications or death.
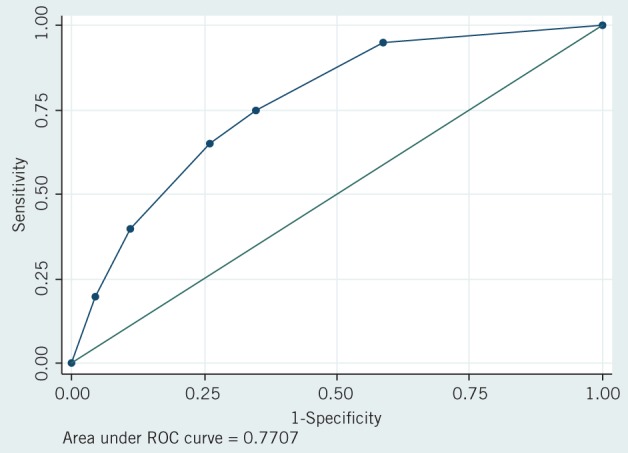
Results: Incidence of major complications was similar in both groups (control: 20/69 [29%], intervention: 23/70 [33%], p=0.622). Immediate admissions to the critical care unit was higher in the intervention group, especially in the SAS 0-4 subgroup (4/6 vs 2/7) although this was not statistically significant (p=0.310). Validity was also confirmed in area under the curve (AUC) analysis (AUC: 0.77).
Conclusions: This pilot study found that a future RCT to investigate the effect of using the SAS in a decisive approach may demonstrate a difference in postoperative care. However, significant changes to the design are needed if differences in clinical outcome are to be achieved reliably. These would include a wider array of postoperative interventions implemented using a quality improvement approach in a stepped wedge cluster design with blinded collection of outcome data.
Figures

References
-
- Ranson JH, Rifkind KM, Roses DF et al Prognostic signs and the role of operative management in acute pancreatitis. Surg Gynecol Obstet 1974; 139: 69–81. - PubMed
-
- Knaus WA, Wagner DP, Draper EA et al The APACHE III prognostic system. Chest 1991; 100: 1,619–1,636. - PubMed
-
- Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993; 270: 2,957–2,963. - PubMed
-
- Barnett S, Moonesinghe SR. Clinical risk scores to guide perioperative management. Postgrad Med J 2011; 87: 535–541. - PubMed
-
- Gawande AA, Kwaan MR, Regenbogen SE et al An Apgar score for surgery. J Am Coll Surg 2007; 204: 201–208. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical