

Hospital-level variation in ICU admission and critical care procedures for patients hospitalized for pulmonary embolism
- PMID: 24992579
- PMCID: PMC4251611
- DOI: 10.1378/chest.14-0059
Hospital-level variation in ICU admission and critical care procedures for patients hospitalized for pulmonary embolism
Abstract
Background: Variation in the use of ICUs for low-risk conditions contributes to health system inefficiency. We sought to examine the relationship between ICU use for patients with pulmonary embolism (PE) and cost, mortality, readmission, and procedure use.
Methods: We performed a retrospective cohort study including 61,249 adults with PE discharged from 263 hospitals in three states between 2007 and 2010. We generated hospital-specific ICU admission rate quartiles and used a series of multilevel models to evaluate relationships between admission rates and risk-adjusted in-hospital mortality, readmission, and costs and between ICU admission rates and several critical care procedures.
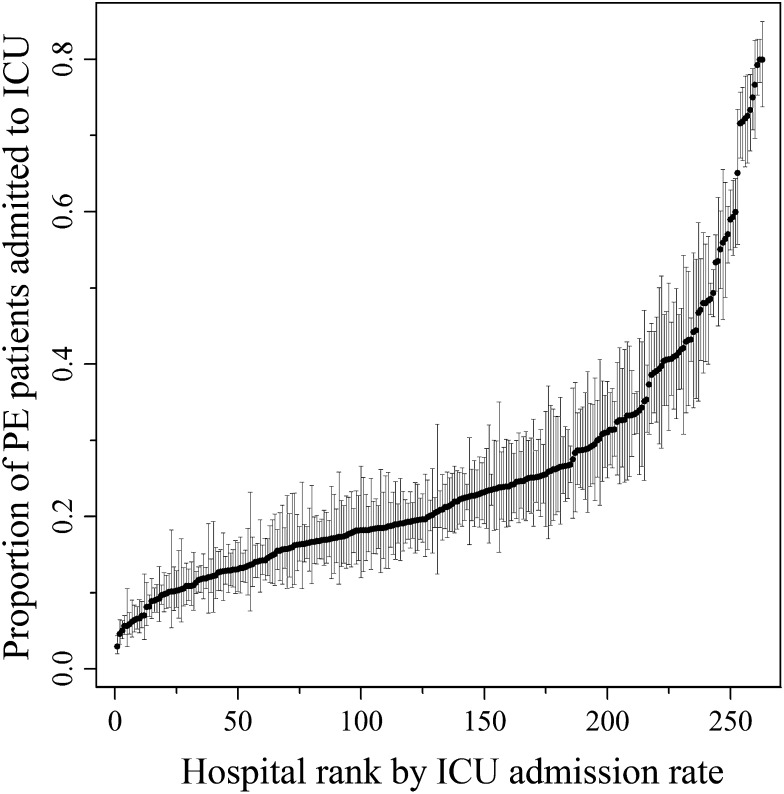
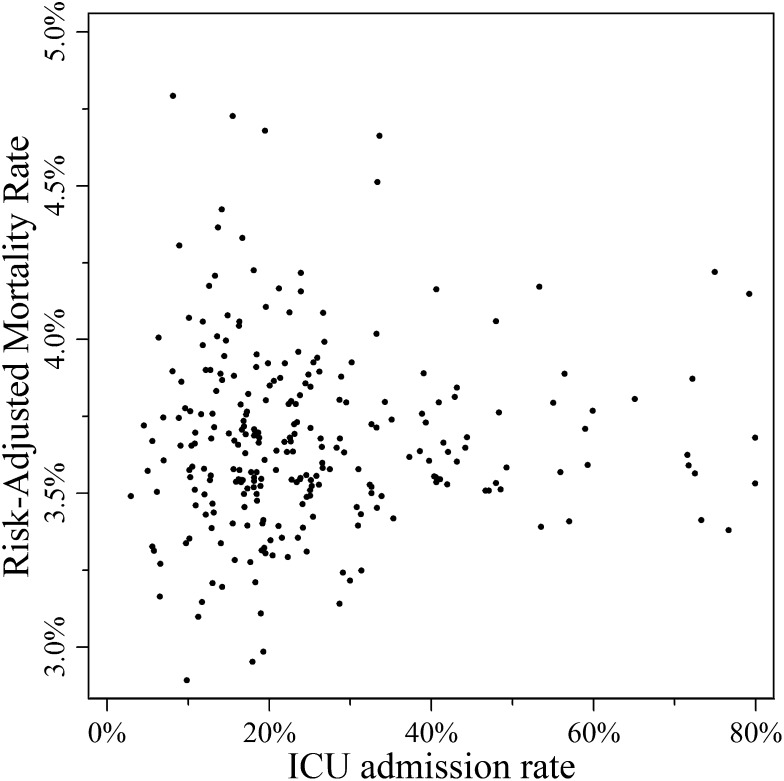
Results: Hospital quartiles varied in unadjusted ICU admission rates for PE (range, ≤ 15% to > 31%). Among all patients, there was a small trend toward increased use of arterial catheterization (0.6%-1.1%, P < .01) in hospital quartiles with higher levels of ICU admission. However, use of invasive mechanical ventilation (14.4%-7.9%, P < .01), noninvasive ventilation (6.6%-3.0%, P < .01), central venous catheterization (14.6%-11.3%, P < .02), and thrombolytics (11.0%-4.7%, P < .01) in patients in the ICU declined across hospital quartiles. There was no relationship between ICU admission rate and risk-adjusted hospital mortality, costs, or readmission.
Conclusions: Hospitals vary widely in ICU admission rates for acute PE without a detectable impact on mortality, cost, or readmission. Patients admitted to ICUs in higher-using hospitals received many critical care procedures less often, suggesting that these patients may have had weaker indications for ICU admission. Hospitals with greater ICU admission may be appropriate targets for improving efficiency in ICU admissions.
Figures
References
-
- Weinberger SE. Providing high-value, cost-conscious care: a critical seventh general competency for physicians. Ann Intern Med. 2011;155(6):386-388. - PubMed
-
- Angus DC, Kelley MA, Schmitz RJ, White A, Popovich J, Jr; Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS). Caring for the critically ill patient. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: can we meet the requirements of an aging population? JAMA. 2000;284(21):2762-2770. - PubMed
-
- Halpern NA, Pastores SM. Critical care medicine in the United States 2000-2005: an analysis of bed numbers, occupancy rates, payer mix, and costs. Crit Care Med. 2010;38(1):65-71. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
