

Time from first presentation in primary care to treatment of symptomatic colorectal cancer: effect on disease stage and survival
- PMID: 24992583
- PMCID: PMC4119995
- DOI: 10.1038/bjc.2014.352
Time from first presentation in primary care to treatment of symptomatic colorectal cancer: effect on disease stage and survival
Abstract
Background: British 5-year survival from colorectal cancer (CRC) is below the European average, but the reasons are unclear. This study explored if longer provider delays (time from presentation to treatment) were associated with more advanced stage disease at diagnosis and poorer survival.
Methods: Data on 958 people with CRC were linked with the Scottish Cancer Registry, the Scottish Death Registry and the acute hospital discharge (SMR01) dataset. Time from first presentation in primary care to first treatment, disease stage at diagnosis and survival time from date of first presentation in primary care were determined. Logistic regression and Cox survival analyses, both with a restricted cubic spline, were used to model stage and survival, respectively, following sequential adjustment of patient and tumour factors.
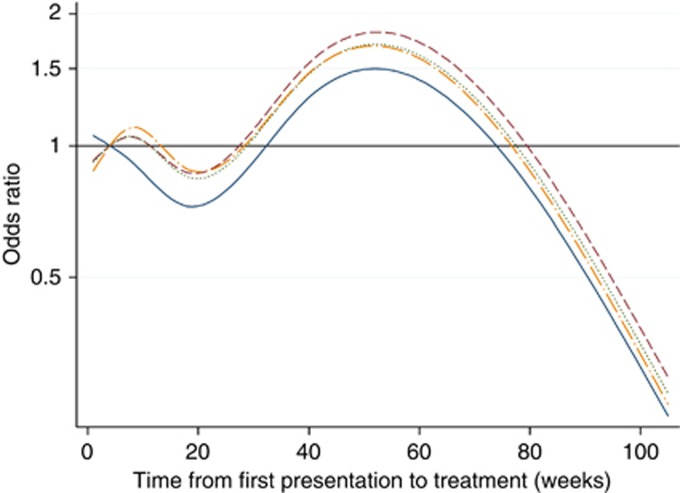
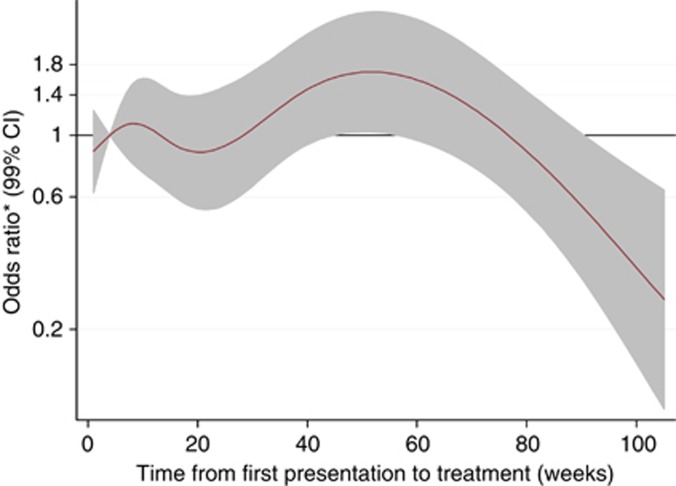
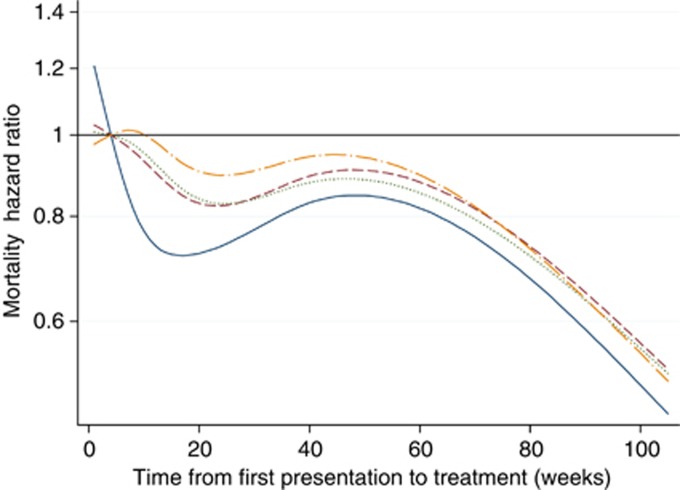
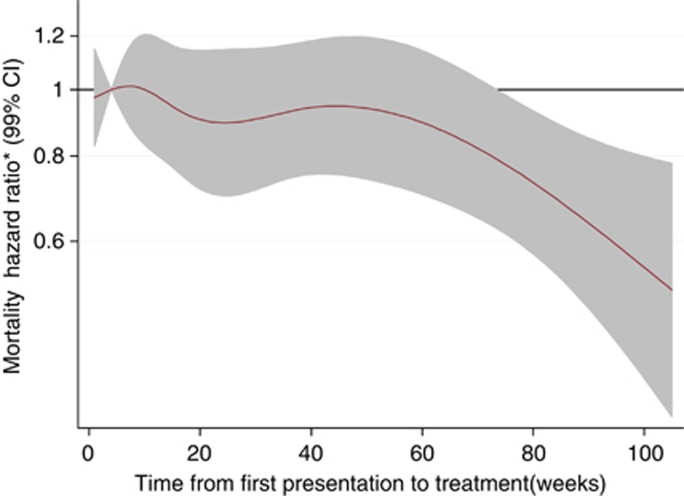
Results: On univariate analysis, those with <4 weeks from first presentation in primary care to treatment had more advanced disease at diagnosis and the poorest prognosis. Treatment delays between 4 and 34 weeks were associated with earlier stage (with the lowest odds ratio occurring at 20 weeks) and better survival (with the lowest hazard ratio occurring at 16 weeks). Provider delays beyond 34 weeks were associated with more advanced disease at diagnosis, but not increased mortality. Following adjustment for patient, tumour factors, emergency admissions and symptoms and signs, no significant relationship between provider delay and stage at diagnosis or survival from CRC was found.
Conclusions: Although allowing for a nonlinear relationship and important confounders, moderately long provider delays did not impact adversely on cancer outcomes. Delays are undesirable because they cause anxiety; this may be fuelled by government targets and health campaigns stressing the importance of very prompt cancer diagnosis. Our findings should reassure patients. They suggest that a health service's primary emphasis should be on quality and outcomes rather than on time to treatment.
Figures
Similar articles
-
Effect of longer health service provider delays on stage at diagnosis and mortality in symptomatic breast cancer.Breast. 2015 Jun;24(3):248-55. doi: 10.1016/j.breast.2015.02.027. Epub 2015 Mar 7. Breast. 2015. PMID: 25753211
-
Time to diagnosis and stage of symptomatic colorectal cancer determined by three different sources of information: A population based retrospective study.Cancer Epidemiol. 2017 Apr;47:48-55. doi: 10.1016/j.canep.2016.10.021. Epub 2017 Jan 23. Cancer Epidemiol. 2017. PMID: 28126583
-
Aspects of survival from colorectal cancer in Denmark.Dan Med J. 2012 Apr;59(4):B4428. Dan Med J. 2012. PMID: 22459726
-
Influence of delay on survival in patients with breast cancer: a systematic review.Lancet. 1999 Apr 3;353(9159):1119-26. doi: 10.1016/s0140-6736(99)02143-1. Lancet. 1999. PMID: 10209974
-
Factors contributing to time to diagnosis in symptomatic colorectal cancer: A scoping review.Eur J Cancer Care (Engl). 2021 May;30(3):e13397. doi: 10.1111/ecc.13397. Epub 2020 Dec 30. Eur J Cancer Care (Engl). 2021. PMID: 33377574
Cited by
-
Consequences of Increasing Time to Colonoscopy Examination After Positive Result From Fecal Colorectal Cancer Screening Test.Clin Gastroenterol Hepatol. 2016 Oct;14(10):1445-1451.e8. doi: 10.1016/j.cgh.2016.05.017. Epub 2016 May 19. Clin Gastroenterol Hepatol. 2016. PMID: 27211498 Free PMC article.
-
Cancer diagnostic tools to aid decision-making in primary care: mixed-methods systematic reviews and cost-effectiveness analysis.Health Technol Assess. 2020 Nov;24(66):1-332. doi: 10.3310/hta24660. Health Technol Assess. 2020. PMID: 33252328 Free PMC article.
-
Treatment delay significantly increases mortality in colorectal cancer: a meta-analysis.Geroscience. 2025 Jun;47(3):5337-5353. doi: 10.1007/s11357-025-01648-z. Epub 2025 Apr 8. Geroscience. 2025. PMID: 40198462 Free PMC article.
-
Cost-effectiveness of FIT and a FIT-based model to optimise symptomatic diagnosis of colorectal cancer: health economic modelling for the COLOFIT project.BMJ Public Health. 2025 Jun 24;3(1):e002089. doi: 10.1136/bmjph-2024-002089. eCollection 2025. BMJ Public Health. 2025. PMID: 40575070 Free PMC article.
-
Impact of SARS-CoV-2 Pandemic on Colorectal Cancer Screening Delay: Effect on Stage Shift and Increased Mortality.Clin Gastroenterol Hepatol. 2021 Jul;19(7):1410-1417.e9. doi: 10.1016/j.cgh.2020.09.008. Epub 2020 Sep 6. Clin Gastroenterol Hepatol. 2021. PMID: 32898707 Free PMC article.
References
-
- Atkin WS, Edwards R, Kralj-Hans I, Wooldrage K, Hart AR, Northover JM, Parkin DM, Wardle J, Duffy SW, Cuzick J. Once-only flexible sigmoidoscopy screening in prevention of CRC: a multicentre randomised controlled trial. Lancet. 2010;375:1624–1633. - PubMed
-
- Brewster DH, Stockton D, Harvey J, Mackay M. Reliability of cancer registration data in Scotland, 1997. Eur J Cancer. 2002;38:414–417. - PubMed
-
- Brewster DH, Stockton DL. Ascertainment of breast cancer by the Scottish Cancer Registry: an assessment based on comparison with five independent breast cancer trials databases. Breast. 2008;17:106–108. - PubMed
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chron Dis. 1987;40:373–383. - PubMed
-
- Department of Health . Cancer Reform Strategy. Department of Health: London, England; 2007.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
