

Kidney function and plasma copeptin levels in healthy kidney donors and autosomal dominant polycystic kidney disease patients
- PMID: 24993447
- PMCID: PMC4152815
- DOI: 10.2215/CJN.08690813
Kidney function and plasma copeptin levels in healthy kidney donors and autosomal dominant polycystic kidney disease patients
Abstract
Background and objectives: Plasma copeptin, a marker of arginine vasopressin, is elevated in patients with autosomal dominant polycystic kidney disease and predicts disease progression. It is unknown whether elevated copeptin levels result from decreased kidney clearance or as compensation for impaired concentrating capacity. Data from patients with autosomal dominant polycystic kidney disease and healthy kidney donors before and after donation were used, because after donation, overall GFR decreases with a functionally normal kidney.
Design, setting, participants, & measurements: Data were obtained between October of 2008 and January of 2012 from healthy kidney donors who visited the institution for routine measurements predonation and postdonation and patients with autosomal dominant polycystic kidney disease who visited the institution for kidney function measurement. Plasma copeptin levels were measured using a sandwich immunoassay, GFR was measured as (125)I-iothalamate clearance, and urine concentrating capacity was measured as urine-to-plasma ratio of urea. In patients with autosomal dominant polycystic kidney disease, total kidney volume was measured with magnetic resonance imaging.
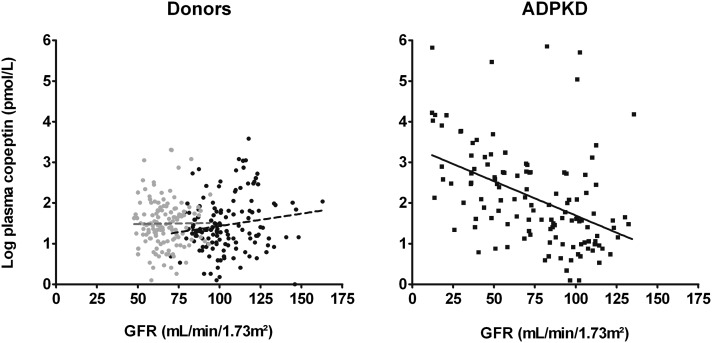
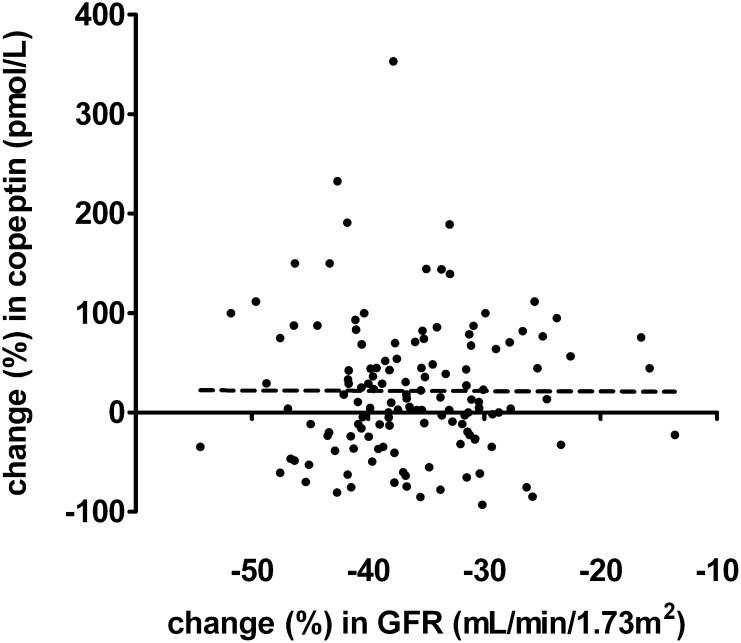
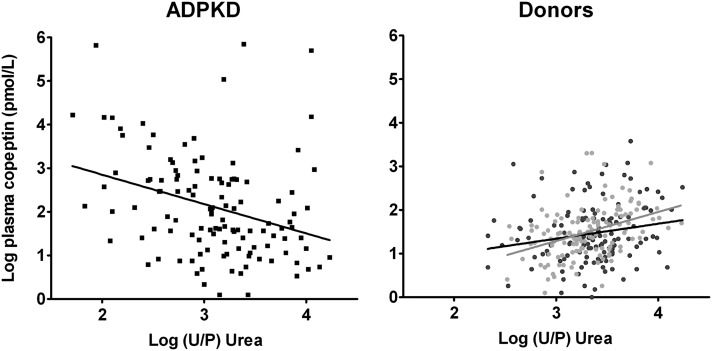
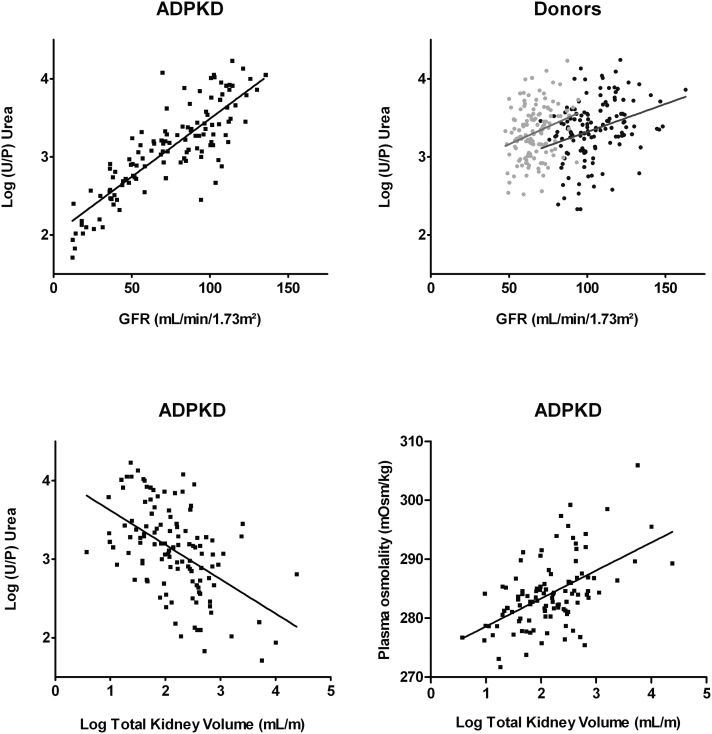
Results: Patients with autosomal dominant polycystic kidney disease (n=122, age=40 years, men=56%) had significantly higher copeptin levels (median=6.8 pmol/L; interquartile range=3.4-15.7 pmol/L) compared with donors (n=134, age=52 years, men=49%) both predonation and postdonation (median=3.8 pmol/L; interquartile range=2.8-6.3 pmol/L; P<0.001; median=4.4 pmol/L; interquartile range=3.6-6.1 pmol/L; P<0.001). In donors, copeptin levels did not change after donation, despite a significant fall in GFR (from 105 ± 17 to 66 ± 10; P<0.001). Copeptin and GFR were significantly associated in patients with autosomal dominant polycystic kidney disease (β=-0.45, P<0.001) but not in donors. In patients with autosomal dominant polycystic kidney disease, GFR and total kidney volume were both associated significantly with urine-to-plasma ratio of urea (β=0.84, P<0.001; β=-0.51, P<0.001, respectively).
Conclusions: On the basis of the finding in donors that kidney clearance is not a main determinant of plasma copeptin levels, it was hypothesized that, in patients with autosomal dominant polycystic kidney disease, kidney damage and associated impaired urine concentration capacity determine copeptin levels.
Keywords: ADPKD; cystic kidney; urea; vasopressin.
Copyright © 2014 by the American Society of Nephrology.
Figures
References
-
- Grantham JJ: Lillian Jean Kaplan International Prize for advancement in the understanding of polycystic kidney disease. Understanding polycystic kidney disease: A systems biology approach. Kidney Int 64: 1157–1162, 2003 - PubMed
-
- Meijer E, Boertien WE, Zietse R, Gansevoort RT: Potential deleterious effects of vasopressin in chronic kidney disease and particularly autosomal dominant polycystic kidney disease. Kidney Blood Press Res 34: 235–244, 2011 - PubMed
-
- Hanaoka K, Guggino WB: cAMP regulates cell proliferation and cyst formation in autosomal polycystic kidney disease cells. J Am Soc Nephrol 11: 1179–1187, 2000 - PubMed
-
- Meijer E, Gansevoort RT, de Jong PE, van der Wal AM, Leonhard WN, de Krey SR, van den Born J, Mulder GM, van Goor H, Struck J, de Heer E, Peters DJ: Therapeutic potential of vasopressin V2 receptor antagonist in a mouse model for autosomal dominant polycystic kidney disease: Optimal timing and dosing of the drug. Nephrol Dial Transplant 26: 2445–2453, 2011 - PubMed
-
- Torres VE, Wang X, Qian Q, Somlo S, Harris PC, Gattone VH, 2nd: Effective treatment of an orthologous model of autosomal dominant polycystic kidney disease. Nat Med 10: 363–364, 2004 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
