

Effect of pre- and post-treatment α-fetoprotein levels and tumor size on survival of patients with hepatocellular carcinoma treated by resection, transarterial chemoembolization or radiofrequency ablation: a retrospective study
- PMID: 24993566
- PMCID: PMC4107750
- DOI: 10.1186/1471-2482-14-40
Effect of pre- and post-treatment α-fetoprotein levels and tumor size on survival of patients with hepatocellular carcinoma treated by resection, transarterial chemoembolization or radiofrequency ablation: a retrospective study
Abstract
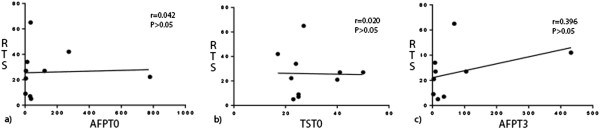
Background: We evaluated treatment modalities and survival in patients with hepatocellular carcinoma (HCC), by pre-treatment and 3-month post-treatment serum alpha-fetoprotein (AFP) levels and pre-treatment tumor diameters.
Methods: We retrospectively reviewed 57 patients treated for HCC in our department from January 2002 to December 2012, including their sex, type of hepatitis, Child class, pre-treatment tumor size, pre-treatment levels of albumin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyltransferase (GGT), red blood cells, hemoglobin, and total bilirubin, pre- and 3-month post-treatment serum AFP, and treatment modality (transarterial chemoembolization, resection or radiofrequency ablation). Survival was analyzed at 1, 3, and 5 years after treatment.
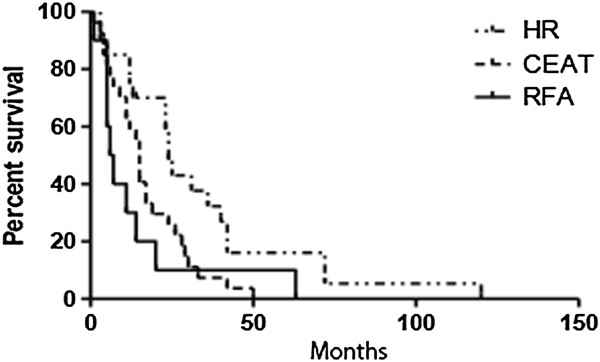
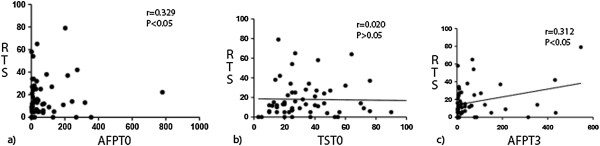
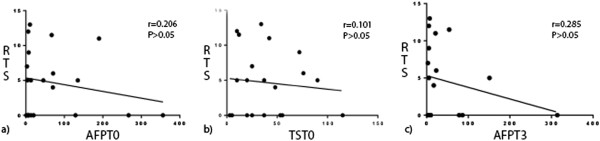
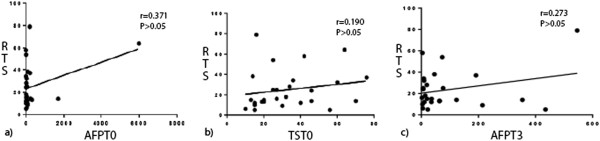
Results: The 57 patients included 44 men and 13 women, of whom 44 had hepatitis C virus (HCV) infection, 3 had hepatitis B virus (HBV) infection, 3 had both HBV and HCV infection, 1 had both HBV and hepatitis D virus infection, and 3 had alcohol-related liver cirrhosis. Both pre- and post-treatment serum AFP levels significantly correlated with recurrent tumor size (P < 0.05 for both). Pre-treatment tumor size did not correlate with recurrent tumor size. Patients who underwent hepatic resection survived significantly longer than those who underwent transarterial chemoembolization or radiofrequency ablation (P < 0.05).
Conclusions: Serum AFP level is useful in diagnosing tumor recurrence and predicting prognosis in HCC patients treated by hepatic resection, transarterial chemoembolization, and radiofrequency ablation. Hepatic resection remains the treatment of choice for HCC in suitable patients.
Figures
References
-
- El-Serag HB. Epidemiology of hepatocellular carcinoma in USA. Hepatol Res. 2007;37(Suppl 2):S88–S94. - PubMed
-
- Zhou YM, Yang JM, Li B, Yin ZF, Xu F, Wang B, Xu W, Kan T. Risk factors for early recurrence of small hepatocellular carcinoma after curative resection. Hepatobiliary Pancreas Dis Int. 2010;9:33–37. - PubMed
-
- Bruix J, Sherman M. Practice Guidelines Committee, American Association for the Study of Liver Diseases Management of hepatocellular carcinoma. Hepatology. 2005;42:1208–1236. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
