

Protocol for a randomised controlled trial of VAsopressin versus Noradrenaline as Initial therapy in Septic sHock (VANISH)
- PMID: 24993769
- PMCID: PMC4091463
- DOI: 10.1136/bmjopen-2014-005866
Protocol for a randomised controlled trial of VAsopressin versus Noradrenaline as Initial therapy in Septic sHock (VANISH)
Abstract
Introduction: Vasopressin is an alternative vasopressor in the management of septic shock. It spares catecholamine use but whether it improves outcome remains uncertain. Current evidence suggests that it may be most effective if used early and possibly in conjunction with corticosteroids. This trial will compare vasopressin to noradrenaline as initial vasopressor in the management of adult septic shock and investigate whether there is an interaction of vasopressin with corticosteroids.
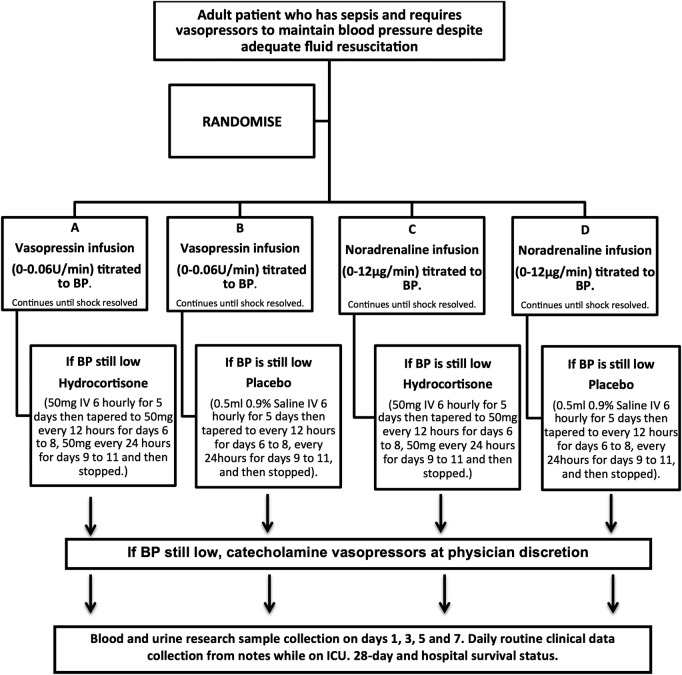
Methods and analysis: This is a multicentre, factorial (2×2), randomised, double-blind, placebo-controlled trial. 412 patients will be recruited from multiple UK intensive care units and randomised to receive vasopressin (0-0.06 U/min) or noradrenaline (0-12 µg/min) as a continuous intravenous infusion as initial vasopressor therapy. If maximum infusion rates of this first study drug are reached, the patient will be treated with either hydrocortisone (initially 50 mg intravenous bolus six-hourly) or placebo, before additional open-label catecholamine vasopressors are prescribed. The primary outcome of the trial will be the difference in renal failure-free days between treatment groups. Secondary outcomes include need for renal replacement therapy, survival rates, other organ failures and resource utilisation.
Ethics and dissemination: The trial protocol and information sheets have received a favourable opinion from the Oxford A Research Ethics Committee (12/SC/0014). There is an independent Data Monitoring and Ethics Committee and independent membership of the Trial Steering Committee including patient and public involvement. The trial results will be published in peer-reviewed journals and presented at national and international scientific meetings.
Trial registration number: ISRCTN 20769191 and EudraCT 2011-005363-24.
Keywords: Statistics & Research Methods.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Hoyert DL, Kung HC, Smith BL. Deaths: preliminary data for 2003. Natl Vital Stat Rep 2005;53:1–48 - PubMed
-
- Vincent JL, Sakr Y, Sprung CL, et al. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med 2006;34:344–53 - PubMed
-
- [No authors listed]. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 1992;20:864–74 - PubMed
-
- Hayes MA, Timmins AC, Yau EH, et al. Elevation of systemic oxygen delivery in the treatment of critically ill patients. N Engl J Med 1994;330:1717–22 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical