

How I do it: lung ultrasound
- PMID: 24993976
- PMCID: PMC4098927
- DOI: 10.1186/1476-7120-12-25
How I do it: lung ultrasound
Abstract
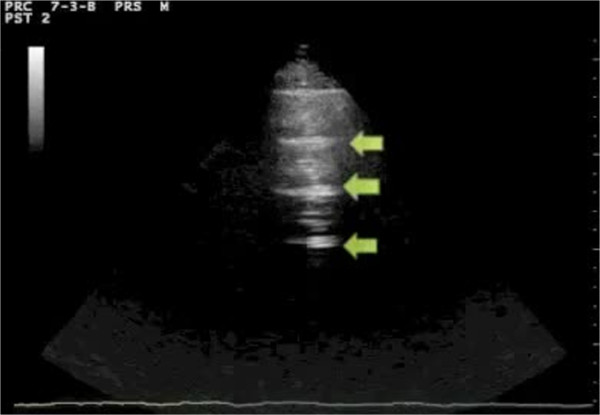
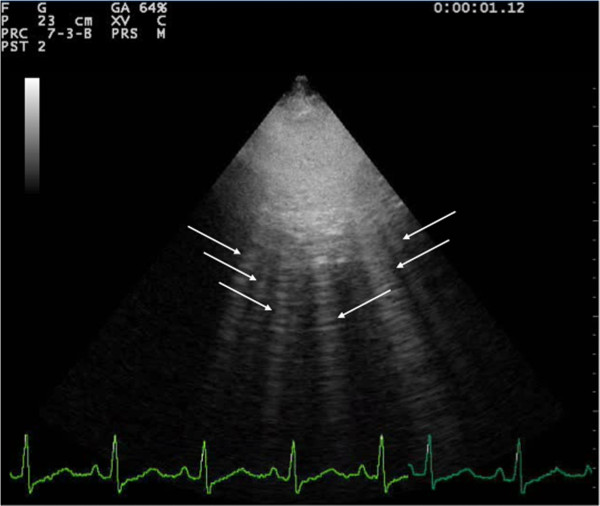
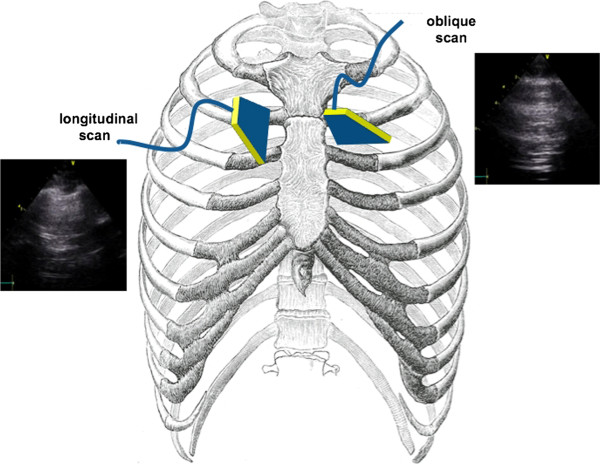
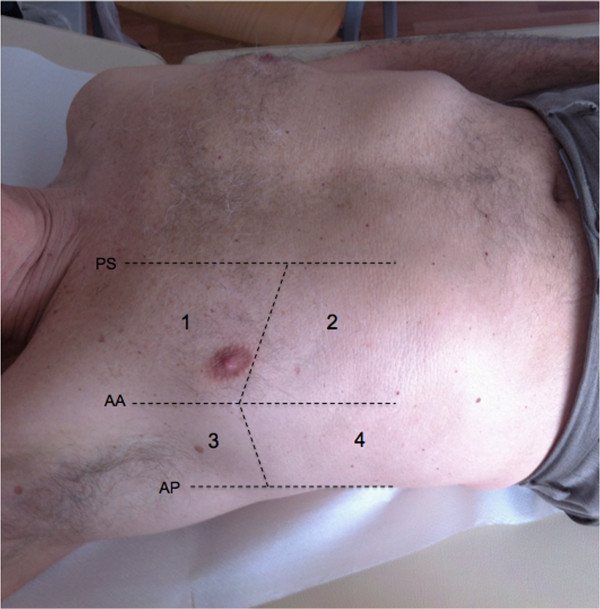
In the last 15 years, a new imaging application of sonography has emerged in the clinical arena: lung ultrasound (LUS). From its traditional assessment of pleural effusions and masses, LUS has moved towards the revolutionary approach of imaging the pulmonary parenchyma, mainly as a point-of-care technique. Although limited by the presence of air, LUS has proved to be useful in the evaluation of many different acute and chronic conditions, from cardiogenic pulmonary edema to acute lung injury, from pneumothorax to pneumonia, from interstitial lung disease to pulmonary infarctions and contusions. It is especially valuable since it is a relatively easy-to-learn application of ultrasound, less technically demanding than other sonographic examinations. It is quick to perform, portable, repeatable, non-ionizing, independent from specific acoustic windows, and therefore suitable for a meaningful evaluation in many different settings, both inpatient and outpatient, in both acute and chronic conditions.In the next few years, point-of-care LUS is likely to become increasingly important in many different clinical settings, from the emergency department to the intensive care unit, from cardiology to pulmonology and nephrology wards.
Figures




References
-
- Longo D, Fauci A, Kasper D, Hauser S, Jameson J, Loscalzo J. Harrison’s Principles of Internal Medicine. 2008.
-
- Volpicelli G. Lung Sonography. J Ultrasound Med. 2013;32:165–171. - PubMed
-
- Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, Melniker L, Gargani L, Noble VE, Via G. others. International Liaison Committee on Lung Ultrasound (ILC-LUS) for Interna tional Consensus Conference on Lung Ultrasound (ICC-LUS). International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012;38:577–591. doi: 10.1007/s00134-012-2513-4. - DOI - PubMed
-
- Ziskin MC, Thickman DI, Goldenberg NJ, Lapayowker MS, Becker JM. The comet tail artifact. J Ultrasound Med. 1982;1(1):1–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
