

Outcome after surgical or conservative management of cerebral cavernous malformations
- PMID: 24994841
- PMCID: PMC4141991
- DOI: 10.1212/WNL.0000000000000684
Outcome after surgical or conservative management of cerebral cavernous malformations
Abstract
Objective: There have been few comparative studies of microsurgical excision vs conservative management of cerebral cavernous malformations (CCM) and none of them has reliably demonstrated a statistically and clinically significant difference.
Methods: We conducted a prospective, population-based study to identify and independently validate definite CCM diagnoses first made in 1999-2003 in Scottish adult residents. We used multiple sources of prospective follow-up to assess adults' dependence and to identify and independently validate outcome events. We used univariate and multivariable survival analyses to test the influence of CCM excision on outcome, adjusted for prognostic factors and baseline imbalances.
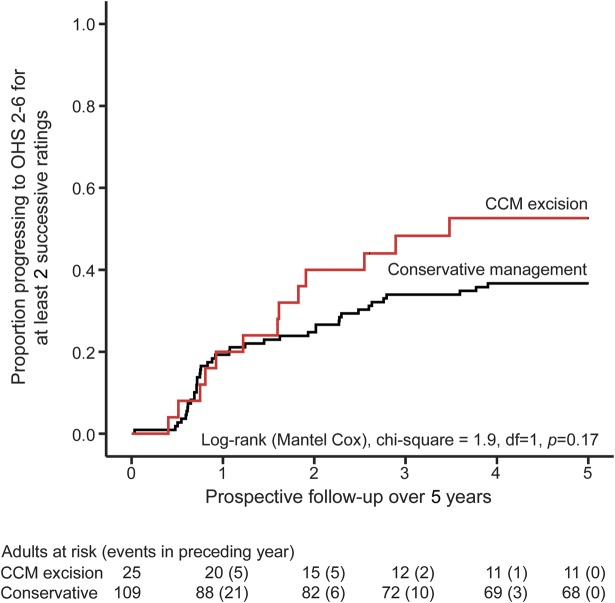
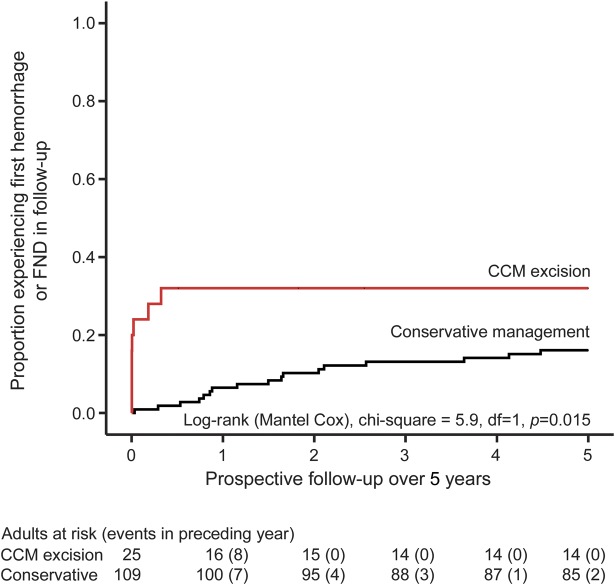
Results: Of 134 adults, 25 underwent CCM excision; these adults were younger (34 vs 43 years at diagnosis, p = 0.004) and more likely to present with symptomatic intracranial hemorrhage or focal neurologic deficit than adults managed conservatively (48% vs 26%; odds ratio 2.7, 95% confidence interval [CI] 1.1-6.5). During 5 years of follow-up, CCM excision was associated with a deterioration to an Oxford Handicap Scale score 2-6 sustained over at least 2 successive years (adjusted hazard ratio [HR] 2.2, 95% CI 1.1-4.3) and the occurrence of symptomatic intracranial hemorrhage or new focal neurologic deficit (adjusted HR 3.6, 95% CI 1.3-10.0).
Conclusions: CCM excision was associated with worse outcomes over 5 years compared to conservative management. Long-term follow-up will determine whether this difference is sustained over patients' lifetimes. Meanwhile, a randomized controlled trial appears justified.
Classification of evidence: This study provides Class III evidence that CCM excision worsens short-term disability scores and increases the risk of symptomatic intracranial hemorrhage and new focal neurologic deficits.
© 2014 American Academy of Neurology.
Figures
Comment in
-
Cavernoma today: keep the surgeon away?Neurology. 2014 Aug 12;83(7):576-7. doi: 10.1212/WNL.0000000000000699. Epub 2014 Jul 3. Neurology. 2014. PMID: 24994840 No abstract available.
References
-
- Flemming KD, Link MJ, Christianson TJ, Brown RD., Jr Prospective hemorrhage risk of intracerebral cavernous malformations. Neurology 2012;78:632–636 - PubMed
-
- Amin-Hanjani S, Ogilvy CS, Ojemann RG, Crowell RM. Risks of surgical management for cavernous malformations of the nervous system. Neurosurgery 1998;42:1220–1227 - PubMed
-
- Ojemann RG, Ogilvy CS. Microsurgical treatment of supratentorial cavernous malformations. Neurosurg Clin N Am 1999;10:433–440 - PubMed
-
- Garrett M, Spetzler RF. Surgical treatment of brainstem cavernous malformations. Surg Neurol 2009;72(suppl 2):S3–S9 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials