

Myocardial bridge as a structure of "double-edged sword" for the coronary artery
- PMID: 24995053
- PMCID: PMC4072857
- DOI: 10.3400/avd.ra.14-00037
Myocardial bridge as a structure of "double-edged sword" for the coronary artery
Abstract
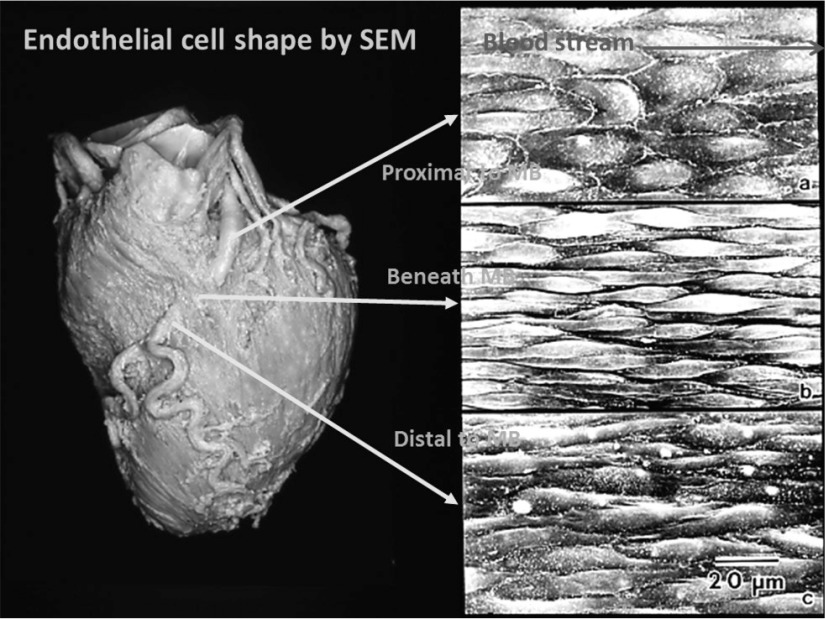
Myocardial bridge (MB) is a chance anatomical structure, comprised of the myocardial tissue, with which the coronary artery running in epicardial adipose tissue is partly covered. It is predominantly present in the left anterior descending artery (LAD) and recognizable through imaging techniques as changes in blood flow within the LAD that arises from MB contraction at cardiac systole. Such changes in blood flow influence the pathophysiology of coronary circulation and atherosclerosis development, thus generating controversy as to whether MB predisposes individual to myocardial infarction (MI). However, recent histomorphometric studies have shown that the individual anatomic properties of MB, such as location, length and thickness, consistently play a critical role in the occurrence of MI. This review article comprehensively addresses the pathophysiological mechanisms of MI occurrence together with the benign suppressive effect of coronary atherosclerosis by MB.
Keywords: atherosclerosis; coronary artery; myocardial bridge; myocardial infarction; pathology.
Figures







Similar articles
-
(1) coronary events caused by myocardial bridge.Ann Vasc Dis. 2009;2(2):79-94. doi: 10.3400/avd.AVDsasvp09001. Epub 2009 Dec 14. Ann Vasc Dis. 2009. PMID: 23555365 Free PMC article.
-
The effects of a myocardial bridge on coronary atherosclerosis and ischaemia.J Pathol. 1998 May;185(1):4-9. doi: 10.1002/(SICI)1096-9896(199805)185:1<4::AID-PATH50>3.0.CO;2-3. J Pathol. 1998. PMID: 9713353 Review.
-
Anatomic properties of myocardial bridge predisposing to myocardial infarction.Circulation. 2009 Aug 4;120(5):376-83. doi: 10.1161/CIRCULATIONAHA.108.820720. Epub 2009 Jul 20. Circulation. 2009. PMID: 19620504
-
Myocardial bridge: a bridge to atherosclerosis.Anadolu Kardiyol Derg. 2007 Mar;7(1):12-6. Anadolu Kardiyol Derg. 2007. PMID: 17347068
-
Significance of the anatomical properties of a myocardial bridge in coronary heart disease.Circ J. 2011;75(7):1559-66. doi: 10.1253/circj.cj-10-1278. Epub 2011 Mar 31. Circ J. 2011. PMID: 21467656 Review.
Cited by
-
Assessment of myocardial bridging and the pericoronary fat attenuation index on coronary computed tomography angiography: predicting coronary artery disease risk.BMC Cardiovasc Disord. 2023 Mar 22;23(1):145. doi: 10.1186/s12872-023-03146-6. BMC Cardiovasc Disord. 2023. PMID: 36949394 Free PMC article.
-
Implications of Myocardial Bridge on Coronary Atherosclerosis and Survival.Diagnostics (Basel). 2022 Apr 10;12(4):948. doi: 10.3390/diagnostics12040948. Diagnostics (Basel). 2022. PMID: 35453995 Free PMC article.
-
Impact of myocardial bridge on lesion morphology and clinical outcomes in patients undergoing IVUS-guided PCI for LAD CTO.Front Cardiovasc Med. 2025 Jul 21;12:1648233. doi: 10.3389/fcvm.2025.1648233. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40761231 Free PMC article.
-
Myocardial bridge over the left anterior descending coronary artery: A case report and review of the literature.J Res Med Sci. 2017 Oct 31;22:113. doi: 10.4103/jrms.JRMS_775_16. eCollection 2017. J Res Med Sci. 2017. PMID: 29184571 Free PMC article.
-
MYOCARDIAL BRIDGE STENTING COMPLICATED BY CORONARY ARTERY PERFORATION AND MIDLAD-RIGHT VENTRICLE FISTULA FORMATION IN NSTEMI PATIENT.Acta Clin Croat. 2024 Mar;63(Suppl1):54-61. doi: 10.20471/acc.2024.63.s1.10. Acta Clin Croat. 2024. PMID: 40599473 Free PMC article.
References
-
- Porstmann W, Iwig J. Intramural coronary vessels in the angiogram. Fortschr Geb Rontgenstr Nuklearmed 1960; 92: 129-33 (in German) - PubMed
-
- Kramer JR, Kitazume H, Proudfit WL, et al. Clinical significance of isolated coronary bridges: benign and frequent condition involving the left anterior descending artery. Am Heart J 1982; 103: 283-8 - PubMed
-
- Stolte M, Weis P, Prestele H. Muscle bridges over the left anterior descending coronary artery: their influence on arterial disease (author’s transl). Virchows Arch A Pathol Anat Histol 1977; 375: 23-36 (in German) - PubMed
-
- Kunkala MR, Schaff HV, Burkhart H, et al. Outcome of repair of myocardial bridging at the time of septal myectomy. Ann Thorac Surg 2014; 97: 118-23 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous