

Pulmonary Langerhans cell histiocytosis: the many faces of presentation at initial CT scan
- PMID: 24996395
- PMCID: PMC4141336
- DOI: 10.1007/s13244-014-0338-0
Pulmonary Langerhans cell histiocytosis: the many faces of presentation at initial CT scan
Abstract
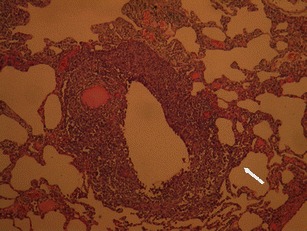
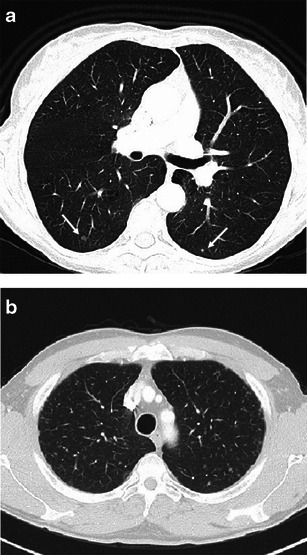
Objectives: Pulmonary Langerhans cell histiocytosis (PLCH) is a rare interstitial granulomatous disease that usually affects young adults who are smokers. Chest computed tomography (CT) allows a confident diagnosis of PLCH only in typical presentation, when nodules, cavitated nodules and cysts coexist and predominate in the upper and middle lungs.
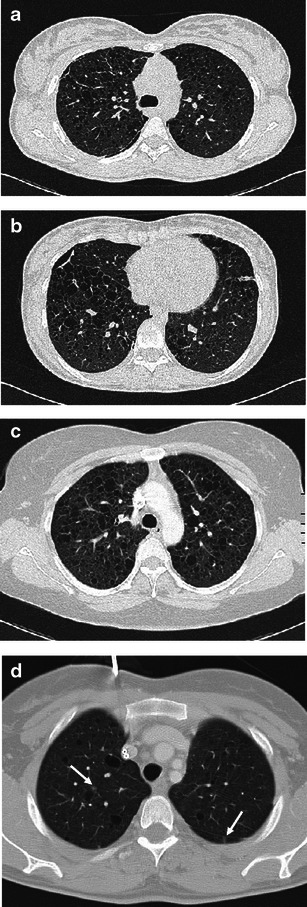
Methods: This article includes a pictorial essay of typical and atypical presentations of PLCH at initial chest CT. Various appearances of PLCH are illustrated and possible differential diagnosis is discussed.
Results: PLCH can present with some aspecific features that may cause diagnosis of the initial disease to be overlooked or other pulmonary diseases to be suspected. In cases of nodule presentation alone, the main differential diagnosis should include lung metastasis, tuberculosis and other infections, sarcoidosis, silicosis and Wegener's disease. In cases of cysts alone, the most common diseases to be differentiated are centrilobular emphysema and lymphangiomyomatosis. Clinical symptoms are usually non-specific, although a history of cigarette smoking, coupled with the presence of typical or suggestive findings at imaging, is key to suspecting the disease. Atypical presentations require surgical biopsy for diagnosis.
Conclusions: The radiologist should be familiar with PLCH imaging features to correctly diagnose the disease or need for further investigation.
Teaching points: • PLCH is a rare interstitial smoking-related disease that usually affects young adults. • The typical first CT shows a mix of nodules, cavitary nodules and cysts in the upper-middle lungs. • Atypical appearance, either cysts or nodules alone, mandates that other diagnoses be considered. • Lung cystic involvement correlates with lung function abnormalities and predicts functional decline. • Integration of the clinical history and imaging results is key to diagnosis.
Figures










References
-
- Weitzman S, Egeler M (2010) Histiocytic disorders of children and adults: basic science, clinical features and therapy, 1st edn. Cambridge University Press, Cambridge, pp 175–224
LinkOut - more resources
Full Text Sources
Other Literature Sources
