

Management of the stiff finger: evidence and outcomes
- PMID: 24996467
- PMCID: PMC4124823
- DOI: 10.1016/j.cps.2014.03.011
Management of the stiff finger: evidence and outcomes
Abstract
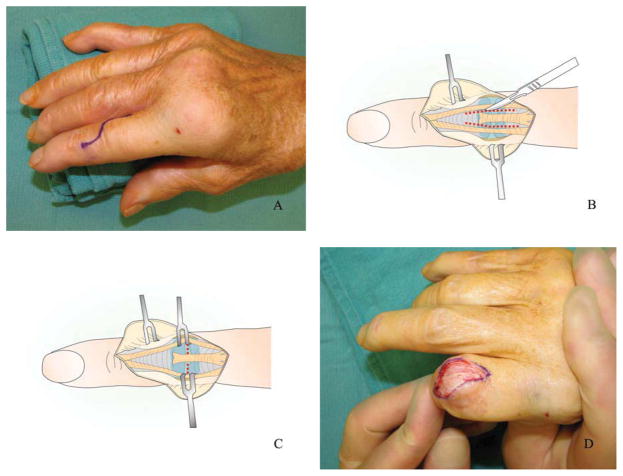
The term "stiff finger" refers to a reduction in the range of motion in the finger. Prevention of stiff fingers by judicious mobilization of the joints is prudent to avoid more complicated treatment after established stiffness occurs. Static progressive and dynamic splints are considered effective non-operative interventions to treat stiff fingers. Capsulotomy and collateral ligament release and other soft tissue release of the MCP and PIP joint are also discussed in this article. Future outcomes research is vital to assessing the effectiveness of these surgical procedures and guiding postoperative treatments.
Keywords: Capsulotomy; Contracture; Finger; Metacarpophalangeal joint; Proximal interphalangeal joint; Splint; Stiffness.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The Pathogenesis and Treatment of the Stiff Finger.Clin Plast Surg. 2019 Jul;46(3):339-345. doi: 10.1016/j.cps.2019.02.007. Epub 2019 Apr 19. Clin Plast Surg. 2019. PMID: 31103078 Review.
-
Contractures of the proximal interphalangeal joint.Hand Clin. 1992 Nov;8(4):777-86. Hand Clin. 1992. PMID: 1460074
-
Management of Flexor Pulley Injuries with Proximal Interphalangeal Joint Contracture.Hand Clin. 2018 May;34(2):251-266. doi: 10.1016/j.hcl.2017.12.001. Hand Clin. 2018. PMID: 29625644 Review.
-
[Contracture release of PIP and MP joints : classification, technique and results].Orthopade. 2008 Dec;37(12):1171-9. doi: 10.1007/s00132-008-1323-4. Orthopade. 2008. PMID: 19048228 German.
-
Neurovascular Advancement Flap to Release Flexion Contracture of the Proximal Interphalangeal Joint.J Hand Surg Am. 2017 Apr;42(4):300.e1-300.e5. doi: 10.1016/j.jhsa.2017.01.007. Epub 2017 Feb 24. J Hand Surg Am. 2017. PMID: 28242241 Review.
Cited by
-
Two-component surface replacement implants compared with perichondrium transplantation for restoration of Metacarpophalangeal and proximal Interphalangeal joints: a retrospective cohort study with a mean follow-up time of 6 respectively 26 years.BMC Musculoskelet Disord. 2020 Oct 7;21(1):657. doi: 10.1186/s12891-020-03687-3. BMC Musculoskelet Disord. 2020. PMID: 33028285 Free PMC article.
-
Outcome of functional treatment with a Lucerne Cast in patients with hand fractures: a retrospective case series.Eur J Trauma Emerg Surg. 2023 Jun;49(3):1555-1560. doi: 10.1007/s00068-023-02234-8. Epub 2023 Feb 9. Eur J Trauma Emerg Surg. 2023. PMID: 36759403
-
A Prospective Study of Contracture of the Finger and its Management in a Tertiary Care Center.Ann Afr Med. 2024 Jul 1;23(3):482-487. doi: 10.4103/aam.aam_153_23. Epub 2024 Jul 20. Ann Afr Med. 2024. PMID: 39034576 Free PMC article.
-
Dynamic External Fixator as Treatment for Congenital Little Finger Contracture.J Hand Microsurg. 2020 Dec 31;15(1):75-79. doi: 10.1055/s-0040-1721563. eCollection 2023 Feb. J Hand Microsurg. 2020. PMID: 36761057 Free PMC article.
-
Reconstruction of finger joints using autologous rib perichondrium - an observational study at a single Centre with a median follow-up of 37 years.BMC Musculoskelet Disord. 2020 Apr 29;21(1):278. doi: 10.1186/s12891-020-03310-5. BMC Musculoskelet Disord. 2020. PMID: 32349740 Free PMC article.
References
-
- Davis TR. Surgical treatment of primary Dupuytren’s contractures of the fingers in the UK: surgeons’ preferences and research priorities. J Hand Surg Eur Vol. 2013;38:83–5. - PubMed
-
- Scott FA, Boswick JA., Jr Palmar arthroplasty for the treatment of the stiff swan-neck deformity. J Hand Surg Am. 1983;8:267–72. - PubMed
-
- Rizio L, Belsky MR. Finger deformities in rheumatoid arthritis. Hand Clin. 1996;12:531–40. - PubMed
-
- Hernández-Cortés P, Caba M, Gómez-Sánchez R, et al. Digital flexion contracture and severe carpal tunnel syndrome due to tophaceus infiltration of wrist flexor tendon: first manifestation of gout. Orthopedics. 2011;34:e797–9. - PubMed
-
- Rosenbloom AL. Limitation of finger joint mobility in diabetes mellitus. J Diabet Complications. 1989;3:77–87. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
