

Patients with repaired tetralogy of Fallot suffer from intra- and inter-ventricular cardiac dyssynchrony: a cardiac magnetic resonance study
- PMID: 24996664
- PMCID: PMC4432392
- DOI: 10.1093/ehjci/jeu123
Patients with repaired tetralogy of Fallot suffer from intra- and inter-ventricular cardiac dyssynchrony: a cardiac magnetic resonance study
Abstract
Aims: Patients with repaired tetralogy of Fallot (rTOF) frequently have right bundle branch block. To better understand the contribution of cardiac dyssynchrony to dysfunction, we developed a method to quantify left (LV), right (RV), and inter-ventricular dyssynchrony using standard cine cardiac magnetic resonance (CMR).
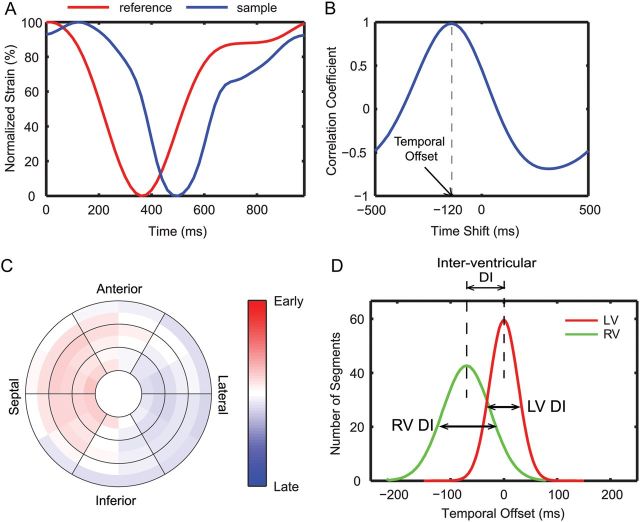
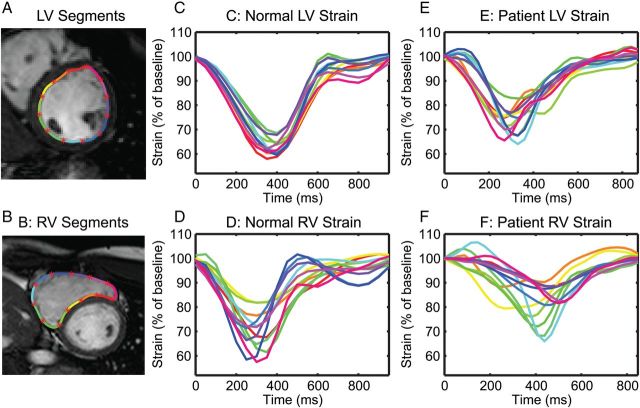
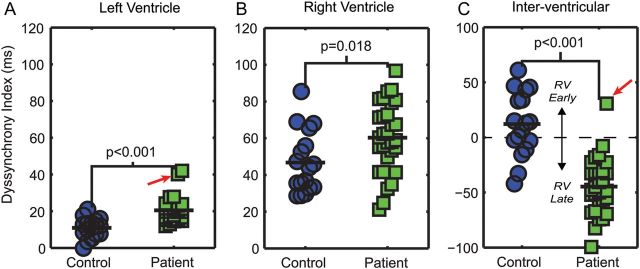
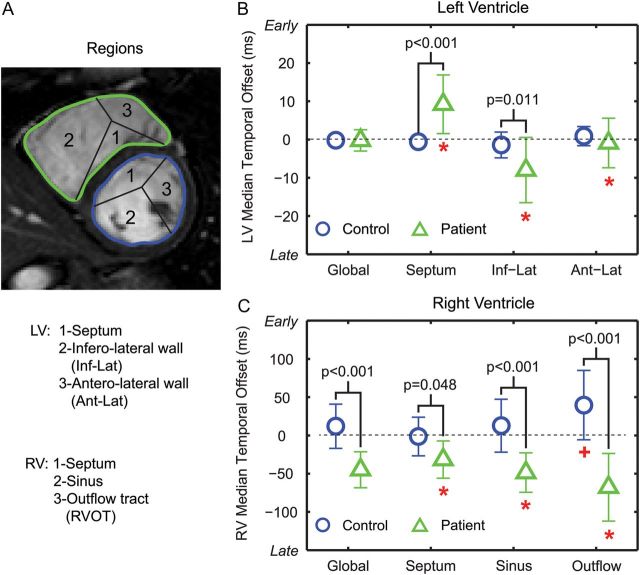
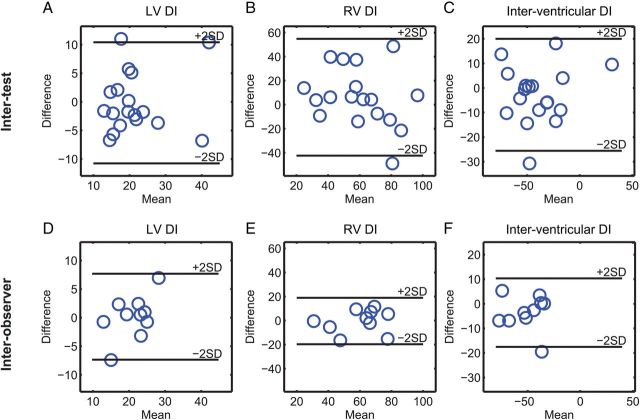
Methods and results: Thirty patients with rTOF and 17 healthy controls underwent cine CMR. Patients were imaged twice to assess inter-test reproducibility. Circumferential strain curves were generated with a custom feature-tracking algorithm for 12 LV and 12 RV segments in each of 4-7 short-axis slices encompassing the ventricles. Temporal offsets (TOs, in ms) of the strain curves relative to a patient-specific reference curve were calculated. The intra-ventricular dyssynchrony index (DI) for each ventricle was computed as the standard deviation of the TOs. The inter-ventricular DI was calculated as the difference in median RV and median LV TOs. Compared with controls, patients had a greater LV DI (21 ± 8 vs. 11 ± 5 ms, P < 0.001) and RV DI (60 ± 19 vs. 47 ± 17 ms, P = 0.02). RV contraction was globally delayed in patients, resulting in a greater inter-ventricular DI with the RV contracting 45 ± 25 ms later than the LV vs. 12 ± 29 ms earlier in controls (P < 0.001). Inter-test reproducibility was moderate with all coefficients of variation ≤22%. Both LV and RV DIs were correlated with measures of LV, but not RV, function.
Conclusion: Patients with rTOF have intra- and inter-ventricular dyssynchrony, which can be quantified from standard cine CMR. This new approach can potentially help determine the contribution of dyssynchrony to ventricular dysfunction in future studies.
Keywords: Cardiac magnetic resonance; Dyssynchrony; Magnetic resonance imaging; Tetralogy of Fallot.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2014. For permissions please email: journals.permissions@oup.com.
Figures



Similar articles
-
Left and right ventricular dyssynchrony and strains from cardiovascular magnetic resonance feature tracking do not predict deterioration of ventricular function in patients with repaired tetralogy of Fallot.J Cardiovasc Magn Reson. 2016 Aug 22;18(1):49. doi: 10.1186/s12968-016-0268-8. J Cardiovasc Magn Reson. 2016. PMID: 27549809 Free PMC article.
-
Mechanisms of right ventricular electromechanical dyssynchrony and mechanical inefficiency in children after repair of tetralogy of fallot.Circ Cardiovasc Imaging. 2014 Jul;7(4):610-8. doi: 10.1161/CIRCIMAGING.113.001483. Epub 2014 May 1. Circ Cardiovasc Imaging. 2014. PMID: 24785673
-
Characteristics of left ventricular dysfunction in repaired tetralogy of Fallot: A multi-institutional deep learning analysis of regional strain and dyssynchrony.J Cardiovasc Magn Reson. 2025 Summer;27(1):101886. doi: 10.1016/j.jocmr.2025.101886. Epub 2025 Mar 21. J Cardiovasc Magn Reson. 2025. PMID: 40122390 Free PMC article.
-
The value of myocardial strain imaging in the evaluation of patients with repaired Tetralogy of Fallot: a review of the literature.Heart Fail Rev. 2023 Jan;28(1):97-112. doi: 10.1007/s10741-022-10223-z. Epub 2022 Mar 14. Heart Fail Rev. 2023. PMID: 35286572 Review.
-
Adverse remodelling in tetralogy of Fallot: From risk factors to imaging analysis and future perspectives.Hellenic J Cardiol. 2024 Jan-Feb;75:48-59. doi: 10.1016/j.hjc.2023.07.008. Epub 2023 Jul 25. Hellenic J Cardiol. 2024. PMID: 37495104 Review.
Cited by
-
Feature tracking CMR reveals abnormal strain in preclinical arrhythmogenic right ventricular dysplasia/ cardiomyopathy: a multisoftware feasibility and clinical implementation study.J Cardiovasc Magn Reson. 2017 Sep 1;19(1):66. doi: 10.1186/s12968-017-0380-4. J Cardiovasc Magn Reson. 2017. PMID: 28863780 Free PMC article.
-
Quantitative Analysis of Electro-Anatomical Maps: Application to an Experimental Model of Left Bundle Branch Block/Cardiac Resynchronization Therapy.IEEE J Transl Eng Health Med. 2016 Dec 16;5:1900215. doi: 10.1109/JTEHM.2016.2634006. eCollection 2017. IEEE J Transl Eng Health Med. 2016. PMID: 29164019 Free PMC article.
-
Subclinical myocardial dysfunction and dyssynchrony after Ross or Ross-Konno procedure.Transl Pediatr. 2020 Apr;9(2):191-194. doi: 10.21037/tp.2020.03.11. Transl Pediatr. 2020. PMID: 32477921 Free PMC article. No abstract available.
-
Comparison of left ventricular strains and torsion derived from feature tracking and DENSE CMR.J Cardiovasc Magn Reson. 2018 Sep 13;20(1):63. doi: 10.1186/s12968-018-0485-4. J Cardiovasc Magn Reson. 2018. PMID: 30208894 Free PMC article.
-
Impact of surgical pulmonary valve replacement on ventricular strain and synchrony in patients with repaired tetralogy of Fallot: a cardiovascular magnetic resonance feature tracking study.J Cardiovasc Magn Reson. 2018 Jun 18;20(1):37. doi: 10.1186/s12968-018-0460-0. J Cardiovasc Magn Reson. 2018. PMID: 29909772 Free PMC article.
References
-
- Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890–900. - PubMed
-
- Nollert G, Fischlein T, Bouterwek S, Bohmer C, Klinner W, Reichart B. Long-term survival in patients with repair of tetralogy of Fallot: 36-year follow-up of 490 survivors of the first year after surgical repair. J Am Coll Cardiol. 1997;30:1374–83. - PubMed
-
- Abd El Rahman MY, Hui W, Yigitbasi M, Dsebissowa F, Schubert S, Hetzer R, et al. Detection of left ventricular asynchrony in patients with right bundle branch block after repair of tetralogy of Fallot using tissue-Doppler imaging-derived strain. J Am Coll Cardiol. 2005;45:915–21. - PubMed
-
- van Oosterhout MF, Prinzen FW, Arts T, Schreuder JJ, Vanagt WYR, Cleutjens JPM, et al. Asynchronous electrical activation induces asymmetrical hypertrophy of the left ventricular wall. Circulation. 1998;98:588–95. - PubMed
-
- Fogel MA, Weinberg PM, Fellows KE, Hoffman EA. A study in ventricular-ventricular interaction. Single right ventricles compared with systemic right ventricles in a dual-chamber circulation. Circulation. 1995;92:219–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
