

Socioeconomic burden of hereditary angioedema: results from the hereditary angioedema burden of illness study in Europe
- PMID: 24996814
- PMCID: PMC4105891
- DOI: 10.1186/1750-1172-9-99
Socioeconomic burden of hereditary angioedema: results from the hereditary angioedema burden of illness study in Europe
Abstract
Background: Hereditary angioedema (HAE) due to C1 inhibitor deficiency is a rare but serious and potentially life-threatening disease marked by spontaneous, recurrent attacks of swelling. The study objective was to characterize direct and indirect resource utilization associated with HAE from the patient perspective in Europe.
Methods: The study was conducted in Spain, Germany, and Denmark to assess the real-world experience of HAE via a cross-sectional survey of HAE patients, including direct and indirect resource utilization during and between attacks for patients and their caregivers over the past 6 months. A regression model examined predictors of medical resource utilization.
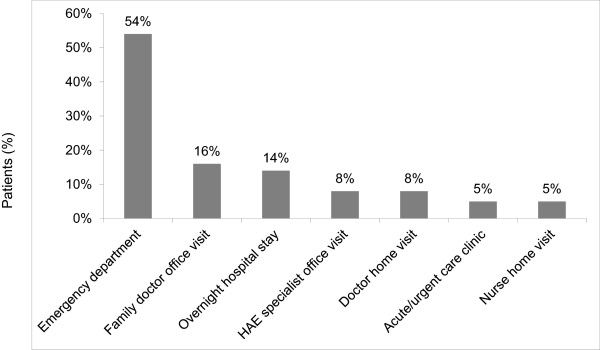
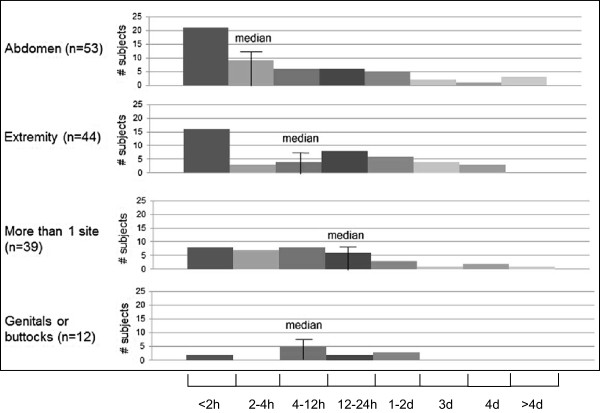
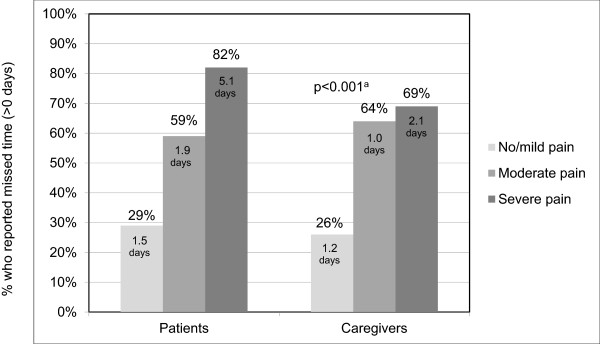
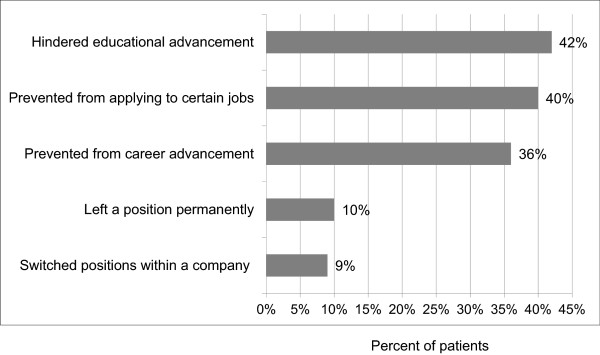
Results: Overall, 164 patients had an attack in the past 6 months and were included in the analysis. The most significant predictor of medical resource utilization was the severity of the last attack (OR 2.6; p < 0.001). Among patients who sought medical care during the last attack (23%), more than half utilized the emergency department. The last attack prevented patients from their normal activities an average of 4-12 hours. Patient and caregiver absenteeism increased with attack severity and frequency. Among patients who were working or in school (n = 120), 72 provided work/school absenteeism data, resulting in an estimated 20 days missing from work/school on average per year; 51% (n = 84) indicated that HAE has hindered their career/educational advancement.
Conclusion: HAE poses a considerable burden on patients and their families in terms of direct medical costs and indirect costs related to lost productivity. This burden is substantial at the time of attacks and in between attacks.
Figures
References
-
- Agostoni A, Cicardi M. Hereditary and acquired C1-inhibitor deficiency: biological and clinical characteristics in 235 patients. Medicine. 1992;71:206–215. - PubMed
-
- Frank MM, Gelfand JA, Atkinson JP. Hereditary angioedema: the clinical syndrome and its management. Ann Intern Med. 1976;84:580–593. - PubMed
-
- Caballero T, Baeza M, Cabanas R, Campos A, Cimbollek S, Gomez-Traseira C, Gonzalez-Quevedo T, Guilarte M, Jurado-Palomo J, Larco JI, Lopez-Serrano MC, Lopez-Trascasa M, Marcos C, Munoz-Caro JM, Pedrosa M, Prior N, Rubio M, Sala-Cunill A. Consensus statement on the diagnosis, management, and treatment of angioedema mediated by bradykinin: part I: classification, epidemiology, pathophysiology, genetics, clinical symptoms, and diagnosis. J Investig Allergol Clin Immunol. 2011;21:333–347. - PubMed
-
- Bork K, Meng G, Staubach P, Hardt J. Hereditary angioedema: new findings concerning symptoms, affected organs, and course. Am J Med. 2006;119:267–274. - PubMed
-
- Bygum A. Hereditary angio-oedema in Denmark: a nationwide survey. Br J Dermatol. 2009;161:1153–1158. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
