

Point-of-care lateral flow assays for tuberculosis and cryptococcal antigenuria predict death in HIV infected adults in Uganda
- PMID: 25000489
- PMCID: PMC4084886
- DOI: 10.1371/journal.pone.0101459
Point-of-care lateral flow assays for tuberculosis and cryptococcal antigenuria predict death in HIV infected adults in Uganda
Abstract
Background: Mortality in hospitalized, febrile patients in Sub-Saharan Africa is high due to HIV-infected, severely immunosuppressed patients with opportunistic co-infection, particularly disseminated tuberculosis (TB) and cryptococcal disease. We sought to determine if a positive lateral flow assay (LFA) result for urine lipoarabinomannan (LAM) and cryptococcal antigenuria was associated with mortality.
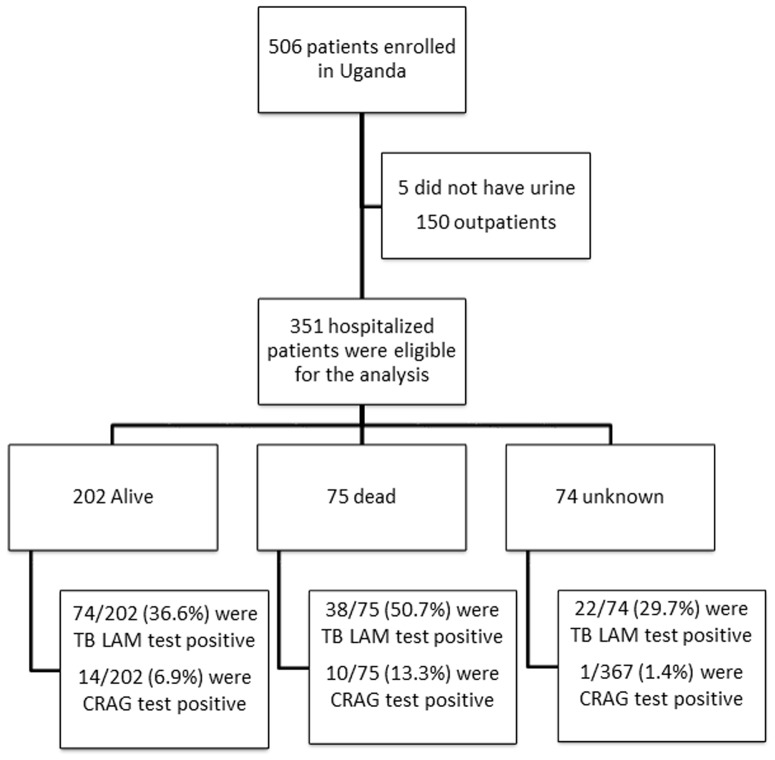
Methods: 351 hospitalized, HIV-positive adults with symptoms consistent with TB and who were able to provide both urine and sputum specimens were prospectively enrolled at Mulago National Referral Hospital in Uganda as part of a prospective accuracy evaluation of the lateral flow Determine TB LAM test. Stored frozen urine was retrospectively tested for cryptococcal antigen (CRAG) using the LFA. We fitted a multinomial logistic regression model to analyze factors associated with death within 2 months after initial presentation.
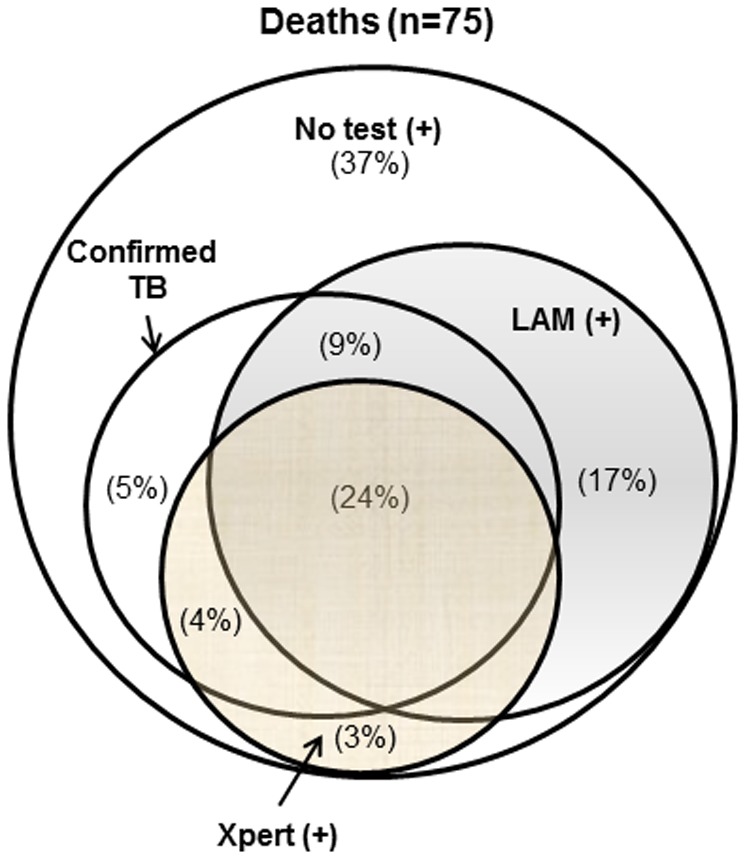
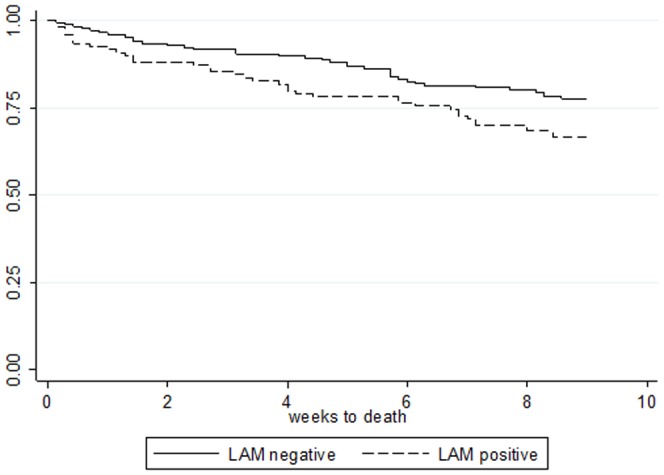
Results: The median CD4 of the participants was 57 (IQR: 14-179) cells/µl and 41% (145) were microbiologically confirmed TB cases. LAM LFA was positive in 38% (134), 7% (25) were CRAG positive, and 43% (151) were positive for either test in urine. Overall, 21% (75) died within the first 2 months, and a total of 32% (114) were confirmed dead by 6 months. At 2 months, 30% of LAM or CRAG positive patients were confirmed dead compared to 15.0% of those who were negative. In an adjusted model, LAM or CRAG positive results were associated with an increased risk of death (RRR 2.29, 95% CI: 1.29, 4.05; P = 0.005).
Conclusions: In hospitalized HIV-infected patients, LAM or CRAG LFA positivity was associated with subsequent death within 2 months. Further studies are warranted to examine the impact of POC diagnostic 'test and treat' approach on patient-centered outcomes.
Conflict of interest statement
Figures
References
-
- Corbett EL, Marston B, Churchyard GJ, De Cock KM (2006) Tuberculosis in sub-Saharan Africa: opportunities, challenges, and change in the era of antiretroviral treatment. Lancet 367: 926–937. - PubMed
-
- Archibald LK, den Dulk MO, Pallangyo KJ, Reller LB (1998) Fatal Mycobacterium tuberculosis bloodstream infections in febrile hospitalized adults in Dar es Salaam, Tanzania. Clin Infect Dis 26: 290–296. - PubMed
-
- Saleri N, Capone S, Pietra V, De Iaco G, Del Punta V, et al. (2009) Outcome and predictive factors of mortality in hospitalized HIV-patients in Burkina Faso. Infection 37: 142–147. - PubMed
-
- Agaba PA, Digin E, Makai R, Apena L, Agbaji OO, et al. (2011) Clinical characteristics and predictors of mortality in hospitalized HIV-infected Nigerians. J Infect Dev Ctries 5: 377–382. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
