

Failure of radioactive iodine in the treatment of hyperthyroidism
- PMID: 25001092
- PMCID: PMC4330099
- DOI: 10.1245/s10434-014-3858-4
Failure of radioactive iodine in the treatment of hyperthyroidism
Abstract
Background: Persistent or recurrent hyperthyroidism after treatment with radioactive iodine (RAI) is common and many patients require either additional doses or surgery before they are cured. The purpose of this study was to identify patterns and predictors of failure of RAI in patients with hyperthyroidism.
Methods: We conducted a retrospective review of patients treated with RAI from 2007 to 2010. Failure of RAI was defined as receipt of additional dose(s) and/or total thyroidectomy. Using a Cox proportional hazards model, we conducted univariate analysis to identify factors associated with failure of RAI. A final multivariate model was then constructed with significant (p < 0.05) variables from the univariate analysis.
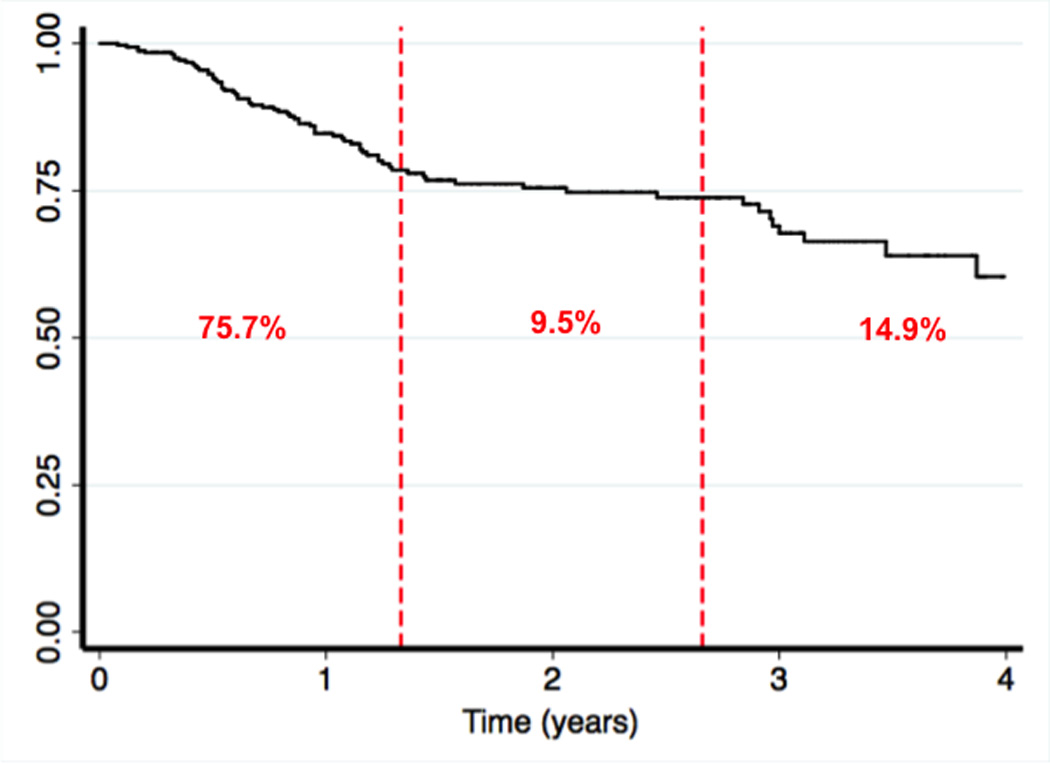
Results: Of the 325 patients analyzed, 74 patients (22.8 %) failed initial RAI treatment, 53 (71.6 %) received additional RAI, 13 (17.6 %) received additional RAI followed by surgery, and the remaining 8 (10.8 %) were cured after thyroidectomy. The percentage of patients who failed decreased in a stepwise fashion as RAI dose increased. Similarly, the incidence of failure increased as the presenting T3 level increased. Sensitivity analysis revealed that RAI doses <12.5 mCi were associated with failure while initial T3 and free T4 levels of at least 4.5 pg/mL and 2.3 ng/dL, respectively, were associated with failure. In the final multivariate analysis, higher T4 (hazard ratio [HR] 1.13; 95 % confidence interval [CI] 1.02-1.26; p = 0.02) and methimazole treatment (HR 2.55; 95 % CI 1.22-5.33; p = 0.01) were associated with failure.
Conclusions: Laboratory values at presentation can predict which patients with hyperthyroidism are at risk for failing RAI treatment. Higher doses of RAI or surgical referral may prevent the need for repeat RAI in selected patients.
Figures
References
-
- Astrup A, Buemann B, Christensen NJ, Madsen J, Gluud C, Bennett P, Svenstrup B. The contribution of body composition, substrates, and hormones to the variability in energy expenditure and substrate utilization in premenopausal women. J Clin Endocrinol Metab. 1992;74(2):279–286. - PubMed
-
- Wilber JF. Thyrotropin releasing hormone: secretion and actions. Annu Rev Med. 1973;24:353–364. - PubMed
-
- Siegel E, Tobias CA. Actions of thyroid hormones on cultured human cells. Nature. 1966;212(5068):1318–1321. - PubMed
-
- Ross DS. Radioiodine therapy for hyperthyroidism. N Engl J Med. 2011;364(6):542–550. - PubMed
-
- Schussler-Fiorenza CM, Bruns CM, Chen H. The surgical management of Graves' disease. J Surg Res. 2006;133(2):207–214. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
