

Multi-institutional assessment of sphincter preservation for rectal cancer
- PMID: 25001097
- PMCID: PMC4251773
- DOI: 10.1245/s10434-014-3882-4
Multi-institutional assessment of sphincter preservation for rectal cancer
Abstract
Background: Sphincter-preserving surgery (SPS) has been proposed as a quality measure for rectal cancer surgery. However, previous studies on SPS rates lack critical clinical characteristics, rendering it unclear if variation in SPS rates is due to unmeasured case-mix differences or surgeons' selection criteria. In this context, we investigate the variation in SPS rates at various practice settings.
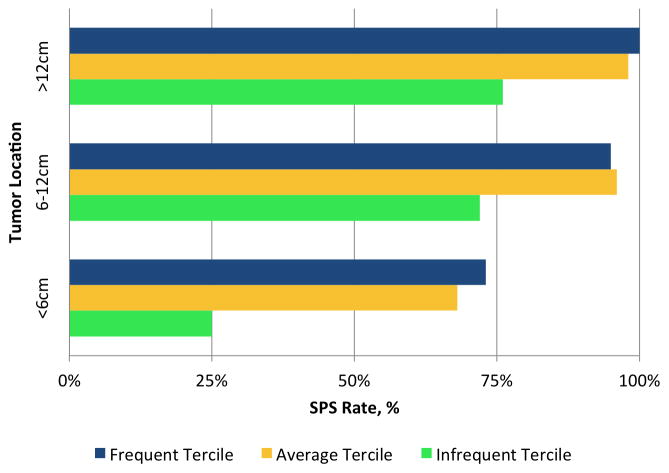
Methods: Ten hospitals in the Michigan Surgical Quality Collaborative collected rectal cancer-specific data, including tumor location and reasons for non-SPS, of patients who underwent rectal cancer surgery from 2007 to 2012. Hospitals were divided into terciles of SPS rates (frequent, average, and infrequent). Patients were categorized as 'definitely SPS eligible' a priori if they did not have any of the following: sphincter involvement, tumor <6 cm from the anal verge, fecal incontinence, stoma preference, or metastatic disease. Fixed-effects logistic regression was used to evaluate for factors associated with SPS.
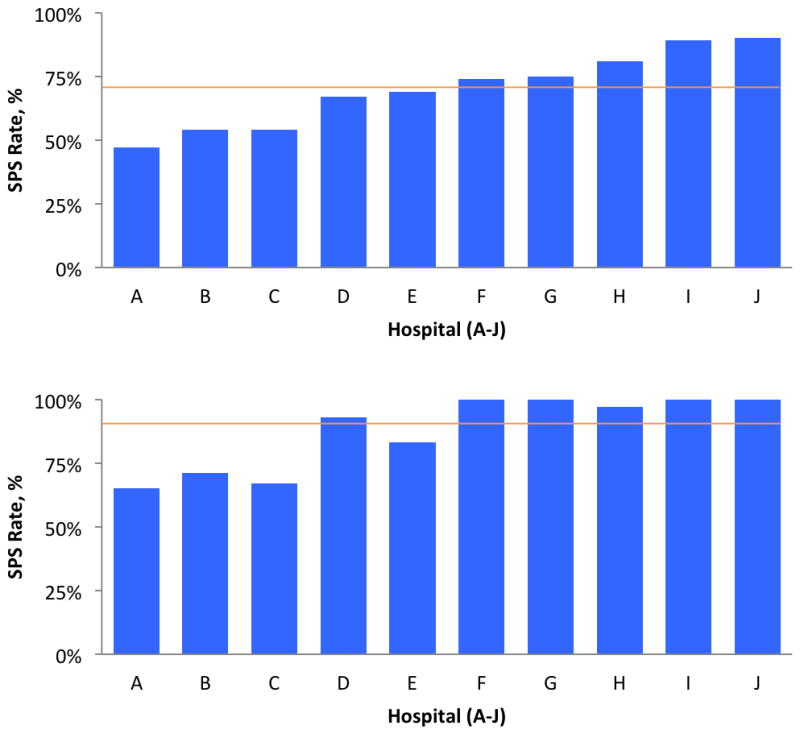
Results: In total, 329 patients underwent rectal cancer surgery at 10 hospitals (5/10 higher volume, and 6/10 major teaching). Overall, 72 % had SPS (range by hospital 47-91 %). Patient and tumor characteristics were similar between hospital terciles. On multivariable analysis, only hospital ID, younger age, and tumor location were associated with SPS, but not sex, race, body mass index, American Joint Committee on Cancer (AJCC) stage, preoperative radiation, or American Society of Anesthesiologists (ASA) class. Analysis of the 181 (55 %) 'definitely-eligible' patients revealed an SPS rate of 90 % (65-100 %).
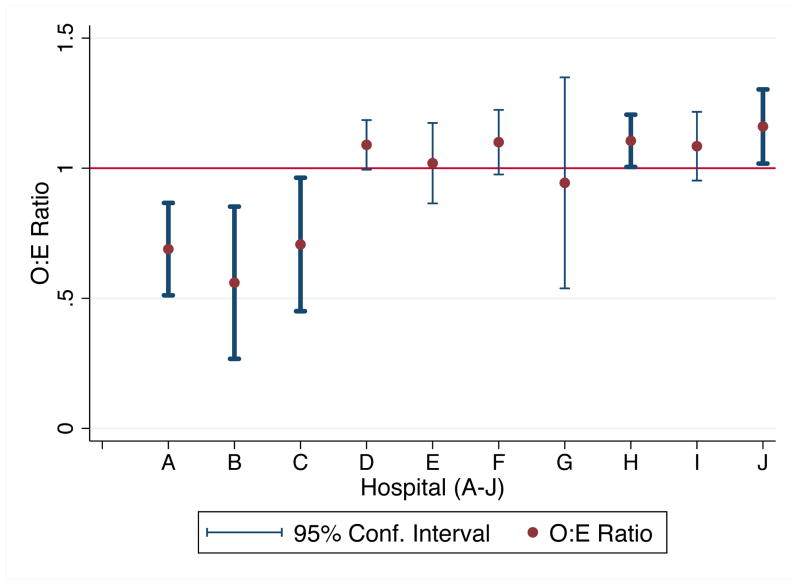
Conclusions: SPS rates vary by hospital, even after accounting for clinical characteristics using detailed chart review. These data suggest missed opportunities for SPS, and refute the general hypothesis that hospital variation in previous studies is due to unmeasured case-mix differences.
Figures
Similar articles
-
Factors associated with sphincter-preserving surgery for rectal cancer at national comprehensive cancer network centers.Ann Surg. 2009 Aug;250(2):260-7. doi: 10.1097/SLA.0b013e3181ae330e. Ann Surg. 2009. PMID: 19638922
-
[Effects of neoadjuvant chemoradiotherapy on the rates of sphincter preserving surgery in lower rectal cancer and analysis of their prognostic factors].Zhonghua Wai Ke Za Zhi. 2016 Jun 1;54(6):419-423. doi: 10.3760/cma.j.issn.0529-5815.2016.06.005. Zhonghua Wai Ke Za Zhi. 2016. PMID: 27938574 Chinese.
-
[Risk factor analysis of low anterior resection syndrome after anal sphincter preserving surgery for rectal carcinoma].Zhonghua Wei Chang Wai Ke Za Zhi. 2017 Mar 25;20(3):289-294. Zhonghua Wei Chang Wai Ke Za Zhi. 2017. PMID: 28338162 Chinese.
-
Sphincter-sparing surgery in patients with low-lying rectal cancer: techniques, oncologic outcomes, and functional results.J Gastrointest Surg. 2014 Jul;18(7):1358-72. doi: 10.1007/s11605-014-2528-y. Epub 2014 May 13. J Gastrointest Surg. 2014. PMID: 24820137 Free PMC article. Review.
-
Sphincter preservation therapy for rectal cancer.Clin Adv Hematol Oncol. 2003 Dec;1(12):735-40. Clin Adv Hematol Oncol. 2003. PMID: 16258478 Review.
Cited by
-
Risk factors influencing sphincter preservation in laparoscopic radical rectal cancer surgery.World J Gastrointest Surg. 2025 Mar 27;17(3):101061. doi: 10.4240/wjgs.v17.i3.101061. World J Gastrointest Surg. 2025. PMID: 40162401 Free PMC article.
-
Hospital variation in sphincter-preservation rates in rectal cancer treatment: results of a population-based study in the Netherlands.BJS Open. 2021 Jul 6;5(4):zrab065. doi: 10.1093/bjsopen/zrab065. BJS Open. 2021. PMID: 34291288 Free PMC article.
-
The fate of preserved sphincter in rectal cancer patients.Int J Colorectal Dis. 2018 Jun;33(6):745-753. doi: 10.1007/s00384-018-3001-2. Epub 2018 Mar 12. Int J Colorectal Dis. 2018. PMID: 29532208
-
Shared Decision-Making, Sphincter Preservation, and Rectal Cancer Treatment: Identifying and Executing What Matters Most to Patients.Clin Colon Rectal Surg. 2023 Jul 19;37(4):256-265. doi: 10.1055/s-0043-1770720. eCollection 2024 Jul. Clin Colon Rectal Surg. 2023. PMID: 38882940 Free PMC article. Review.
-
Trends and outcomes of sphincter-preserving surgery for rectal cancer: a national cancer database study.Int J Colorectal Dis. 2019 Feb;34(2):239-245. doi: 10.1007/s00384-018-3171-y. Epub 2018 Oct 2. Int J Colorectal Dis. 2019. PMID: 30280252
References
-
- Monson JRT, Weiser MR, Buie WD, Chang GJ, Rafferty JF, Buie WD, et al. Practice parameters for the management of rectal cancer (revised) Dis Colon Rectum. 2013 May;56(5):535–50. - PubMed
-
- Temple LK, Romanus D, Niland J, Veer A, Ter Weiser MR, Skibber J, et al. Factors associated with sphincter-preserving surgery for rectal cancer at national comprehensive cancer network centers. Ann Surg. 2009 Aug;250(2):260–7. - PubMed
-
- Ricciardi R, Virnig Ba, Madoff RD, Rothenberger Da, Baxter NN. The status of radical proctectomy and sphincter-sparing surgery in the United States. Dis Colon Rectum. 2007 Aug;50(8):1119–27. discussion 1126–7. - PubMed
-
- Richardson DP, Porter Ga, Johnson PM. Population-based use of sphincter-preserving surgery in patients with rectal cancer: is there room for improvement? Dis Colon Rectum. 2013 Jun;56(6):704–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
