

Confocal laser endomicroscopy of bladder and upper tract urothelial carcinoma: a new era of optical diagnosis?
- PMID: 25002073
- PMCID: PMC4382365
- DOI: 10.1007/s11934-014-0437-y
Confocal laser endomicroscopy of bladder and upper tract urothelial carcinoma: a new era of optical diagnosis?
Abstract
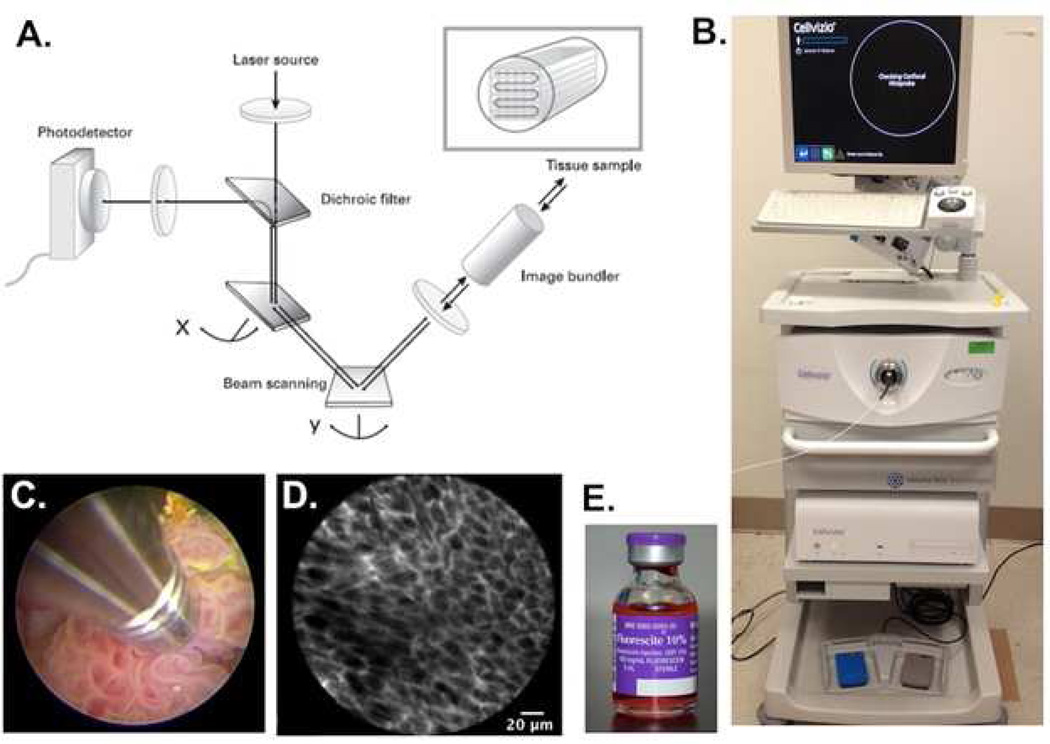
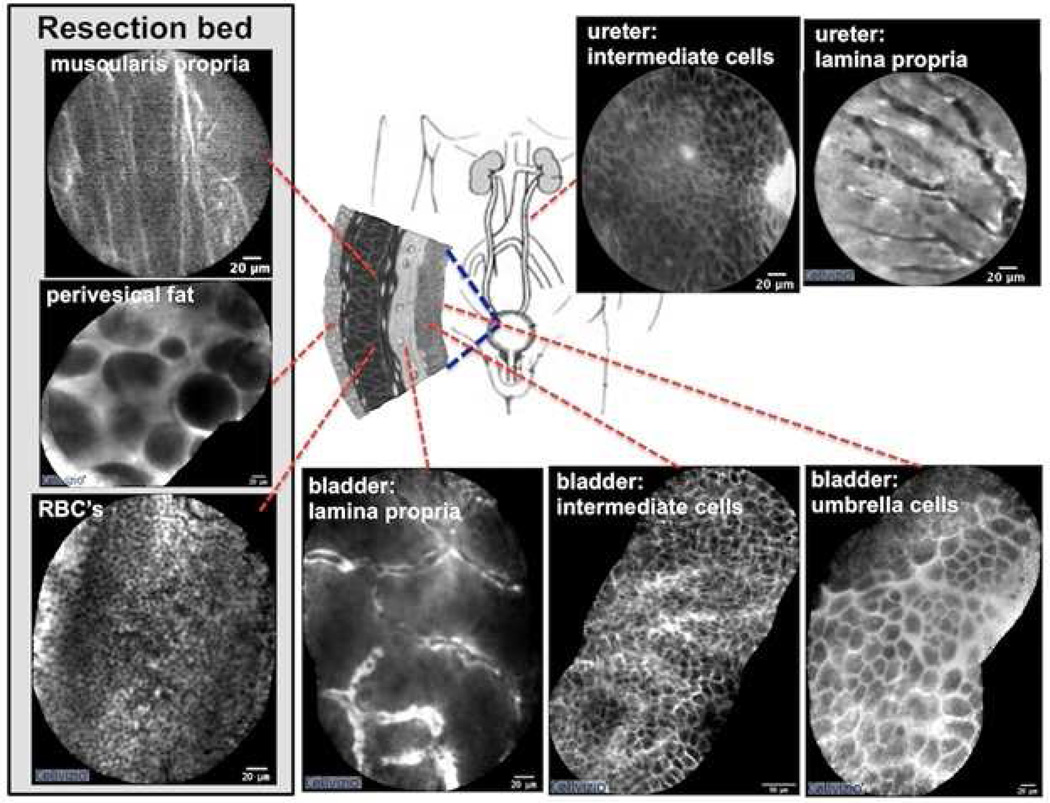
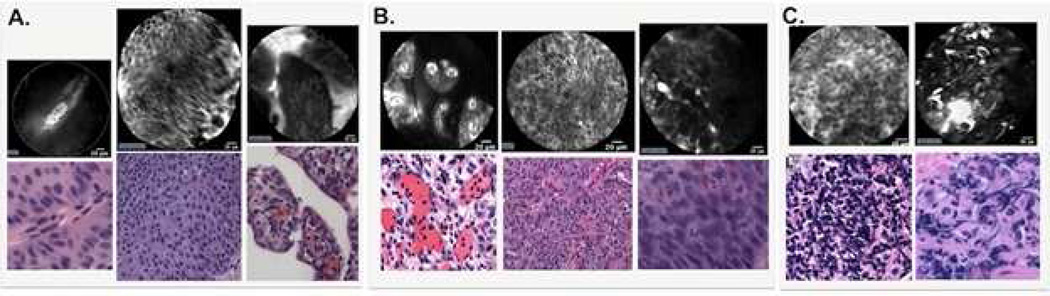
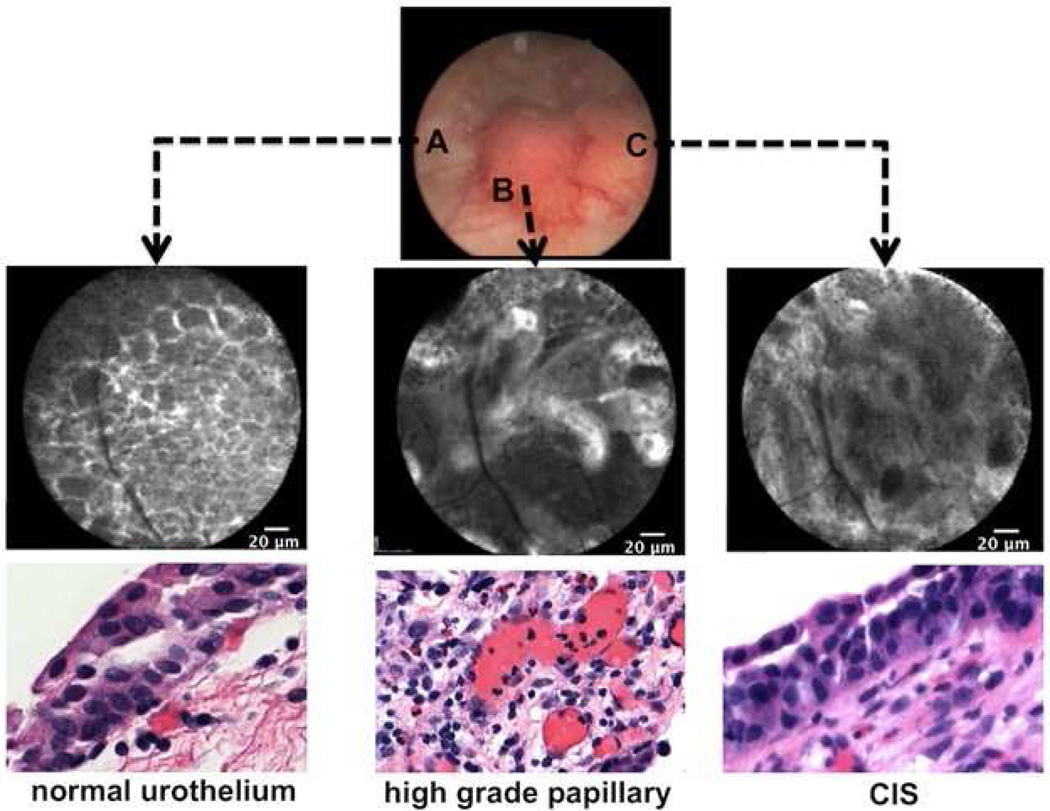
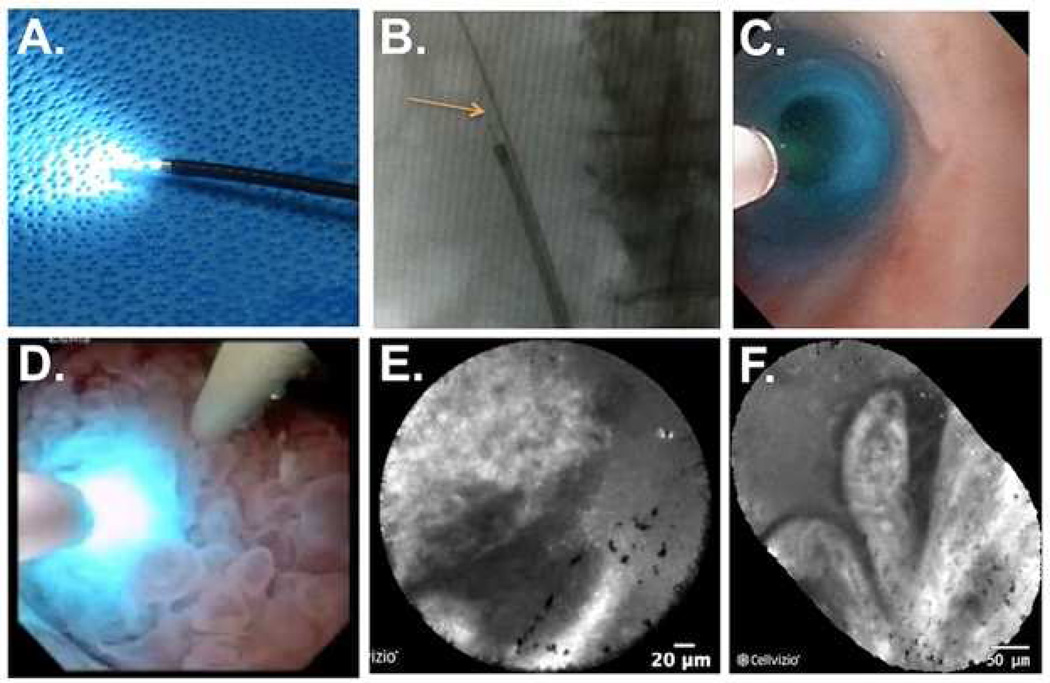
Urothelial carcinoma of the bladder and upper tract pose significant diagnostic and therapeutic challenges. White light endoscopy plays a central role in the management of urothelial carcinoma but has several well-recognized shortcomings. New optical imaging technologies may improve diagnostic accuracy, enhance local cancer control, and better stratify treatment options. Confocal laser endomicroscopy enables dynamic imaging of the cellular structures below the mucosal surface and holds promise in providing real time optical diagnosis and grading of urothelial carcinoma. A variety of imaging probes are available that are compatible with the full spectrum of cystoscopes and ureteroscopes. We review the underlying principles and technique of confocal laser endomicroscopy in the urinary tract, with emphasis on specific application towards urothelial carcinoma. While the available data are largely related to urothelial carcinoma of the bladder, the lessons learned are directly applicable to the upper tract, where the clinical needs are significant. Ongoing efforts to optimize this technology offer an exciting glimpse into future advances in optical imaging and intraoperative image guidance.
Conflict of interest statement
Dr. Stephanie P. Chen and Dr. Joseph C. Liao each declare no potential conflicts of interest.
Figures

References
-
- U.S. Cancer Statistics Working Group. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; 2013. United States Cancer Statistics, 1999–2010 Incidence and Mortality Web-based Report.
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA. Cancer J. Clin. 2014;64:9–29. - PubMed
-
- Kirkali Z, et al. Bladder cancer: epidemiology, staging and grading, and diagnosis. Urology. 2005;66:4–34. - PubMed
-
- Morgan TM, Clark PE. Bladder cancer. Curr. Opin. Oncol. 2010;22:242–249. - PubMed
-
- Sylvester RJ, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur. Urol. 2006;49:466–465. discussion 475–477. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
