

Characteristics and long-term follow-up of participants with peripheral arterial disease during ALLHAT
- PMID: 25002161
- PMCID: PMC4238201
- DOI: 10.1007/s11606-014-2947-1
Characteristics and long-term follow-up of participants with peripheral arterial disease during ALLHAT
Abstract
Background: Hypertension is a major risk factor for peripheral artery disease (PAD). Little is known about relative efficacy of antihypertensive treatments for preventing PAD.
Objectives: To compare, by randomized treatment groups, hospitalized or revascularized PAD rates and subsequent morbidity and mortality among participants in the Antihypertensive and Lipid-Lower Treatment to Prevent Heart Attack Trial (ALLHAT).
Design: Randomized, double-blind, active-control trial in high-risk hypertensive participants.
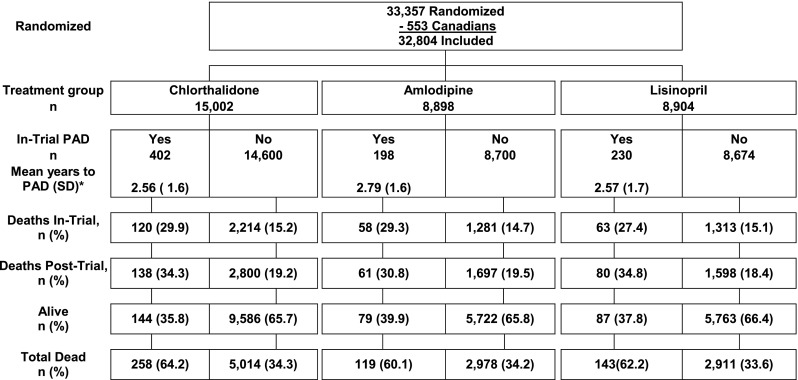
Participants: Eight hundred thirty participants with specified secondary outcome of lower extremity PAD events during the randomized phase of ALLHAT.
Interventions/events: In-trial PAD events were reported during ALLHAT (1994-2002). Post-trial mortality data through 2006 were obtained from administrative databases. Mean follow-up was 8.8 years.
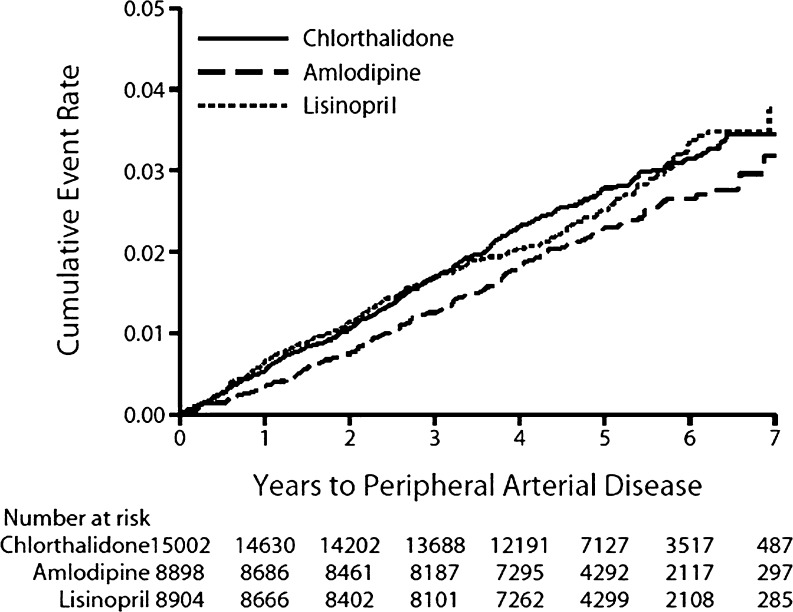
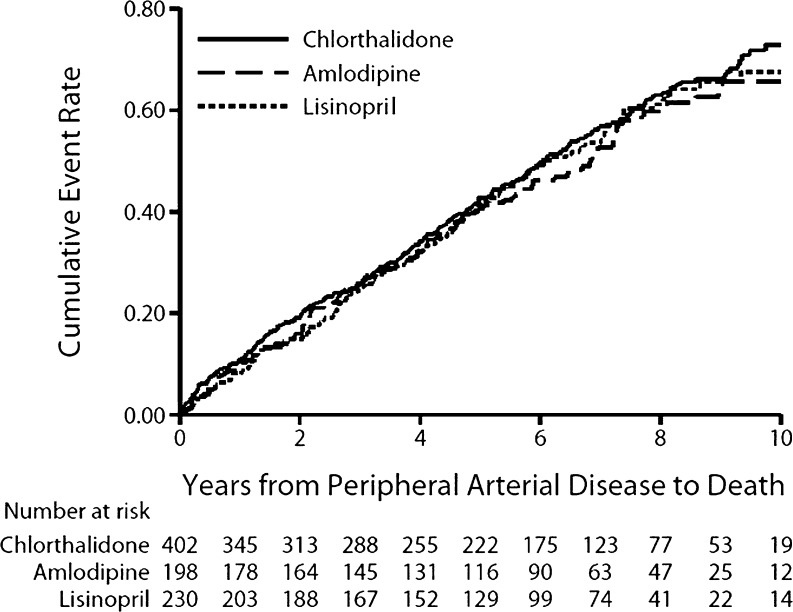
Main measures: Baseline characteristics and intermediate outcomes in three treatment groups, using the Kaplan-Meier method to calculate cumulative event rates and post-PAD mortality rates, Cox proportional hazards regression model for hazard ratios and 95 % confidence intervals, and multivariate Cox regression models to examine risk differences among treatment groups.
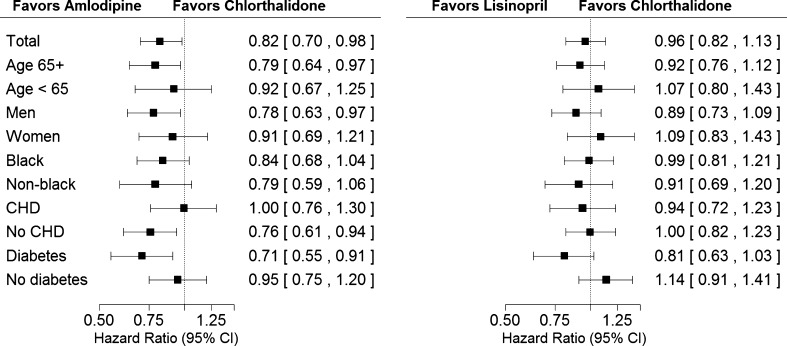
Key results: Following adjustment for baseline characteristics, neither participants assigned to the calcium-channel antagonist amlodipine nor to the ACE-inhibitor lisinopril showed a difference in risk of clinically advanced PAD compared with those in the chlorthalidone arm (HR, 0.86; 95 % CI, 0.72-1.03 and HR, 0.98; 95 % CI, 0.83-1.17, respectively). Of the 830 participants with in-trial PAD events, 63 % died compared to 34 % of those without PAD; there were no significant treatment group differences for subsequent nonfatal myocardial infarction, coronary revascularizations, strokes, heart failure, or mortality.
Conclusions: Neither amlodipine nor lisinopril showed superiority over chlorthalidone in reducing clinically advanced PAD risk. These findings reinforce the compelling need for comparative outcome trials examining treatment of PAD in high-risk hypertensive patients. Once PAD develops, cardiovascular event and mortality risk is high, regardless of type of antihypertensive treatment.
Trial registration: ClinicalTrials.gov NCT00000542.
Figures
Comment in
-
Capsule commentary on Piller et al., Characteristics and long-term follow-up of participants with peripheral vascular disease during ALLHAT.J Gen Intern Med. 2014 Nov;29(11):1527. doi: 10.1007/s11606-014-2983-x. J Gen Intern Med. 2014. PMID: 25092015 Free PMC article. No abstract available.
References
-
- Bozkurt AK, Tasci I, Tabak O, Gumus M, Kaplan Y. Peripheral artery disease assessed by ankle-brachial index in patients with established cardiovascular disease or at least one risk factor for atherothrombosis–CAREFUL study: a national, multi-center, cross-sectional observational study. BMC Cardiovasc Disord. 2011;11:4. doi: 10.1186/1471-2261-11-4. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
