

Impact of clinical decision support on receipt of antibiotic prescriptions for acute bronchitis and upper respiratory tract infection
- PMID: 25002458
- PMCID: PMC4215050
- DOI: 10.1136/amiajnl-2014-002648
Impact of clinical decision support on receipt of antibiotic prescriptions for acute bronchitis and upper respiratory tract infection
Abstract
Objective: Antibiotics are commonly recognized as non-indicated for acute bronchitis and upper respiratory tract infection (URI), yet their widespread use persists. Clinical decision support in the form of electronic warnings is hypothesized to prevent non-indicated prescriptions. The purpose of this study was to identify the effect of clinical decision support on a common type of non-indicated prescription.
Materials and methods: Using National Ambulatory Medical Care Survey data from 2006 to 2010, ambulatory visits with a primary diagnosis of acute bronchitis or URI and orders for antibiotic prescriptions were identified. Visits were classified on the basis of clinician report of decision-support use. Generalized estimating equations were used to assess the effect of decision support on likelihood of antibiotic prescription receipt, controlling for patient, provider, and practice characteristics.
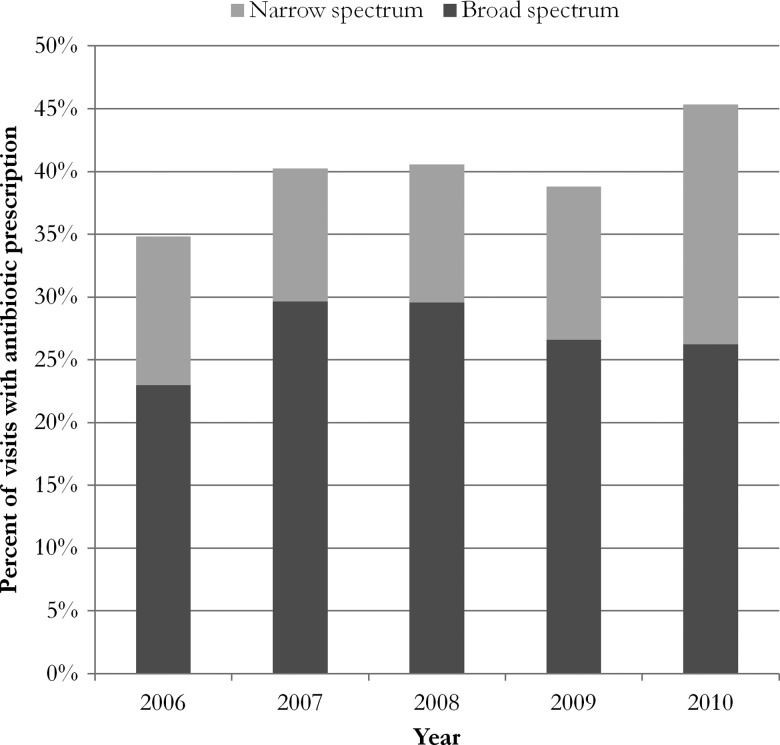
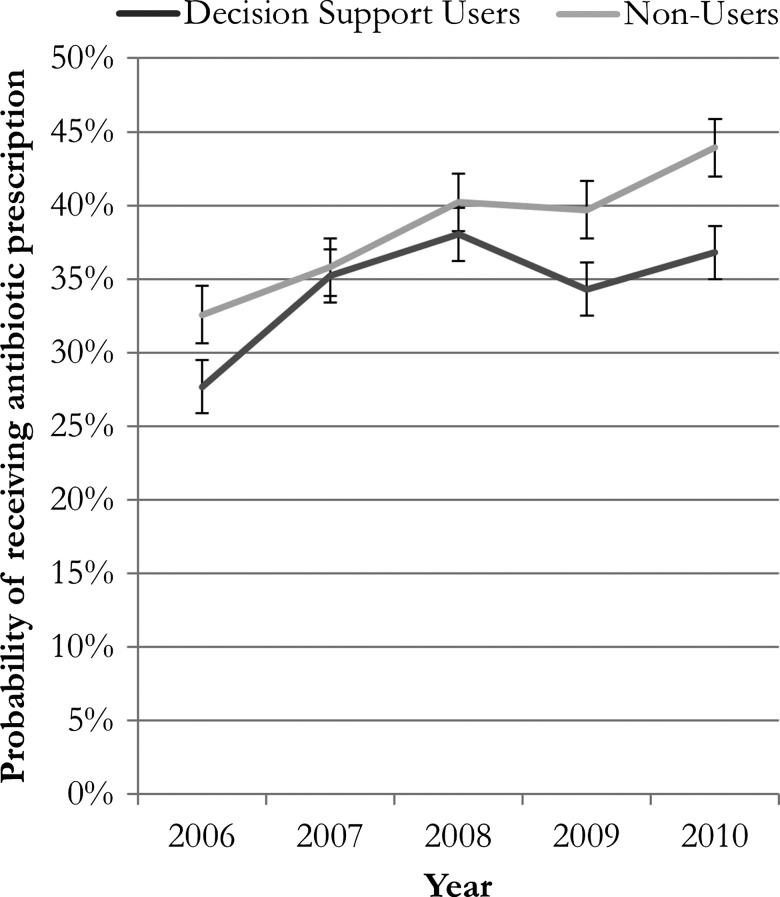
Results: Clinician use of decision support increased sharply between 2006 (16% of visits) and 2010 (55%). Antibiotic prescribing for acute bronchitis and URI increased from ∼35% of visits in 2006 to ∼45% by 2010. Use of decision support was associated with a 19% lower likelihood of receiving an antibiotic prescription, controlling for patient, provider, and practice characteristics.
Discussion: In spite of the increased use of decision-support systems and the relatively fewer non-indicated antibiotic prescriptions resulting from the use of decision support, a secular upward trend in non-indicated antibiotic prescribing offset these improvements.
Conclusions: The overall effect of decision support suggests an important role for technology in reducing non-indicated prescriptions. Decision support alone may not be sufficient to eliminate non-indicated prescriptions given secular trends.
Keywords: Acute bronchitis; Antibiotics; Health information technology.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
Similar articles
-
Antibiotic prescribing for adults with colds, upper respiratory tract infections, and bronchitis by ambulatory care physicians.JAMA. 1997 Sep 17;278(11):901-4. JAMA. 1997. PMID: 9302241
-
Antibiotic prescribing for children with colds, upper respiratory tract infections, and bronchitis.JAMA. 1998 Mar 18;279(11):875-7. doi: 10.1001/jama.279.11.875. JAMA. 1998. PMID: 9516004
-
Ambulatory antibiotic prescribing for acute bronchitis and cough and hospital admissions for respiratory infections: time trends analysis.J R Soc Med. 2006 Jul;99(7):358-62. doi: 10.1177/014107680609900719. J R Soc Med. 2006. PMID: 16816266 Free PMC article.
-
Antimicrobial prescription pattern and appropriateness for respiratory tract infection in outpatients: a systematic review and meta-analysis.Syst Rev. 2024 Sep 6;13(1):229. doi: 10.1186/s13643-024-02649-3. Syst Rev. 2024. PMID: 39243046 Free PMC article.
-
How, why and when are delayed (back-up) antibiotic prescriptions used in primary care? A realist review integrating concepts of uncertainty in healthcare.BMC Public Health. 2024 Oct 14;24(1):2820. doi: 10.1186/s12889-024-20248-8. BMC Public Health. 2024. PMID: 39402467 Free PMC article. Review.
Cited by
-
E-Health Tools to Improve Antibiotic Use and Resistances: A Systematic Review.Antibiotics (Basel). 2020 Aug 12;9(8):505. doi: 10.3390/antibiotics9080505. Antibiotics (Basel). 2020. PMID: 32806583 Free PMC article. Review.
-
Impact of Clinical Decision Support on Antibiotic Prescribing for Acute Respiratory Infections: a Cluster Randomized Implementation Trial.J Gen Intern Med. 2020 Nov;35(Suppl 2):788-795. doi: 10.1007/s11606-020-06096-3. Epub 2020 Sep 1. J Gen Intern Med. 2020. PMID: 32875505 Free PMC article. Clinical Trial.
-
Computerized Clinical Decision Support: Contributions from 2014.Yearb Med Inform. 2015 Aug 13;10(1):119-24. doi: 10.15265/IY-2015-036. Yearb Med Inform. 2015. PMID: 26293858 Free PMC article. Review.
-
Reducing antibiotic prescriptions for respiratory tract infections in family practice: results of a cluster randomized controlled trial evaluating a multifaceted peer-group-based intervention.NPJ Prim Care Respir Med. 2016 Feb 4;26:15083. doi: 10.1038/npjpcrm.2015.83. NPJ Prim Care Respir Med. 2016. PMID: 26845640 Free PMC article. Clinical Trial.
-
Overtreatment in the United States.PLoS One. 2017 Sep 6;12(9):e0181970. doi: 10.1371/journal.pone.0181970. eCollection 2017. PLoS One. 2017. PMID: 28877170 Free PMC article.
References
-
- Yu DT, Seger DL, Lasser KE, et al. . Impact of implementing alerts about medication black-box warnings in electronic health records. Pharmacoepidemiol Drug Saf 2011;20:192–202 - PubMed
-
- Smith DH, Perrin N, Feldstein A, et al. . The impact of prescribing safety alerts for elderly persons in an electronic medical record: an interrupted time series evaluation. Arch Intern Med 2006;166:1098–104 - PubMed
-
- Dowell SF, Marcy SM, Phillips WR, et al. . Principles of judicious use of antimicrobial agents for pediatric upper respiratory tract infections. Pediatrics 1998;101(Suppl 1): 163–5
-
- Gonzales R, Bartlett JG, Besser RE, et al. . Principles of appropriate antibiotic use for treatment of uncomplicated acute bronchitis: background. Ann Intern Med 2001;134:521–9 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
