

Intracranial nonvestibular neurinomas: Young neurosurgeons' experience
- PMID: 25002761
- PMCID: PMC4078606
- DOI: 10.4103/0976-3147.133566
Intracranial nonvestibular neurinomas: Young neurosurgeons' experience
Abstract
Background and objectives: Neurinoma arising from other than nonvestibular cranial nerves is less prevalent. Here we present our experiences regarding the clinical profile, investigations, microneurosurgical management, and the outcome of nonvestibular cranial nerve neurinomas.
Materials and methods: From January 2005 to December 2011, the recorded documents of operated nonvestibular intracranial neurinomas were retrospectively studied for clinical profile, investigations, microneurosurgical management, complications, follow-up, and outcomes.
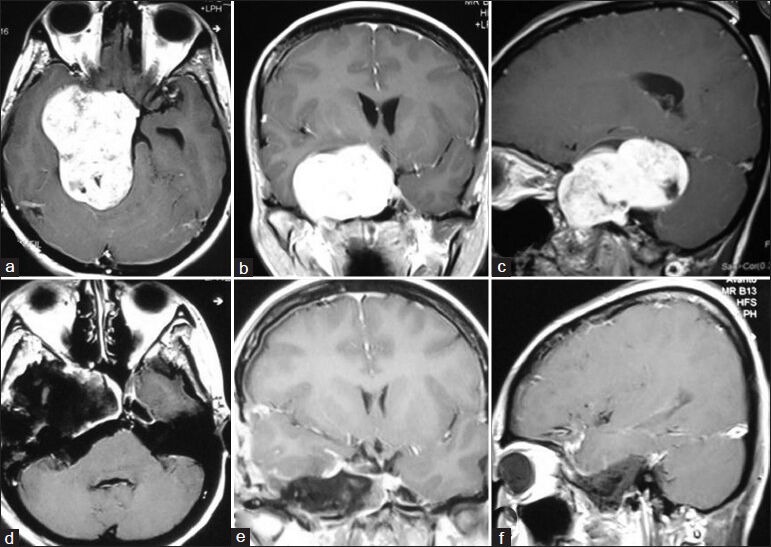
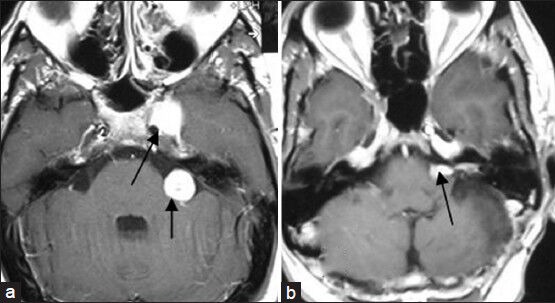
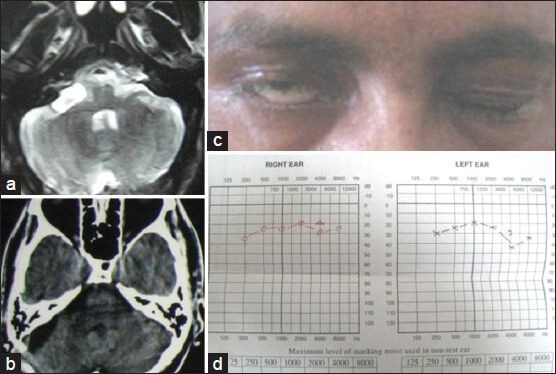
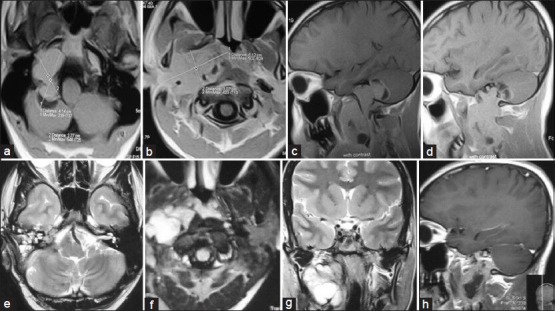
Results: The average follow-up was 24.5 months. Total number of cases was 30, with age ranging from 9 to 60 years. Sixteen cases were males and 14 were females. Nonvestibular cranial nerve schwannomas most commonly originated from trigeminal nerve followed by glossopharyngeal+/vagus nerve. There were three abducent nerve schwannomas that are very rare. There was no trochlear nerve schwannoma. Two glossopharyngeal+/vagus nerve schwannomas extended into the neck through jugular foramen and one extended into the upper cervical spinal canal. Involved nerve dysfunction was a common clinical feature except in trigeminal neurinomas where facial pain was a common feature. Aiming for no new neurodeficit, total resection of the tumor was done in 24 cases, and near-total resection or gross total resection or subtotal resection was done in 6 cases. Preoperative symptoms improved or disappeared in 25 cases. New persistent deficit occurred in 3 cases. Two patients died postoperatively. There was no recurrence of tumor till the last follow-up.
Conclusion: Nonvestibular schwannomas are far less common, but curable benign lesions. Surgical approach to the skull base and craniovertebral junction is a often complex and lengthy procedure associated with chances of significant morbidity. But early diagnosis, proper investigations, and evaluation, along with appropriate decision making and surgical planning with microsurgical techniques are the essential factors that can result in optimum outcome.
Keywords: Intracranial; microneurosurgical management; neurilemmomas; neurinomas; nonvestibular; schwannomas.
Conflict of interest statement
Figures





Similar articles
-
Stereotactic radiosurgery: the preferred management for patients with nonvestibular schwannomas?Int J Radiat Oncol Biol Phys. 2002 Mar 15;52(4):1002-7. doi: 10.1016/s0360-3016(01)02711-0. Int J Radiat Oncol Biol Phys. 2002. PMID: 11958895
-
Nonvestibular schwannomas of the brain: a 7-year experience.Neurosurgery. 2002 Mar;50(3):437-48; discussion 438-9. doi: 10.1097/00006123-200203000-00002. Neurosurgery. 2002. PMID: 11841710
-
Rare Cranial Nerve Schwannomas: A Retrospective Review of Nontrigeminal, Nonvestibular Cranial Nerve Schwannomas.J Neurosci Rural Pract. 2018 Apr-Jun;9(2):258-263. doi: 10.4103/jnrp.jnrp_469_17. J Neurosci Rural Pract. 2018. PMID: 29725180 Free PMC article.
-
Stereotactic radiosurgery for nonvestibular schwannomas.Neurosurg Clin N Am. 2013 Oct;24(4):531-42. doi: 10.1016/j.nec.2013.05.003. Epub 2013 Aug 2. Neurosurg Clin N Am. 2013. PMID: 24093571 Review.
-
Surgical management of jugular foramen schwannomas with hearing and facial nerve function preservation: a series of 23 cases and review of the literature.Laryngoscope. 2006 Dec;116(12):2191-204. doi: 10.1097/01.mlg.0000246193.84319.e5. Laryngoscope. 2006. PMID: 17146395 Review.
Cited by
-
[Extra-axial tumors of the central nervous system].Radiologe. 2017 Sep;57(9):715-727. doi: 10.1007/s00117-017-0291-2. Radiologe. 2017. PMID: 28812110 Review. German.
-
Imaging of Skull Base Tumors.Tomography. 2023 Jun 21;9(4):1196-1235. doi: 10.3390/tomography9040097. Tomography. 2023. PMID: 37489465 Free PMC article. Review.
-
Anatomic location and route of extension of the trigeminal nerve schwannomas.J Neurosci Rural Pract. 2015 Apr-Jun;6(2):280-1. doi: 10.4103/0976-3147.153241. J Neurosci Rural Pract. 2015. PMID: 25883504 Free PMC article. No abstract available.
References
-
- Acharya R, Husain S, Chhabra SS, Patir R, Bhalla S, Seghal AD. Sixth nerve schwannoma: A case report and literature review. Neurol Sci. 2003;24:74–9. - PubMed
-
- Kim DS, Choi JU, Yang KH, Jung JM. Optic sheath schwannoma: Report of two cases. Childs Nerv Syst. 2002;18:684–9. - PubMed
-
- Vachata P, Sames M. Abducens nerve schwannoma mimicking intrinsic brainstem tumor. Acta Neurochir (Wien) 1991;151:1281–7. - PubMed
-
- Ginsberg F, Peyster RG, Rose WS, Drapkin AJ. Sixth nerves schwannoma: MR and CT demonstration. J Comput Assist Tomogr. 1998;12:482–4. - PubMed
-
- Okura A, Shigemori M, Abe T, Yamashita M, Kojima K, Noguchi S. Hemiatrophy of the tongue due to hypoglossal schwannoma shown by MRI. Neuroradiology. 1994;36:239–40. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources