

Altered oscillatory cerebral blood flow velocity and autoregulation in postural tachycardia syndrome
- PMID: 25002851
- PMCID: PMC4067089
- DOI: 10.3389/fphys.2014.00234
Altered oscillatory cerebral blood flow velocity and autoregulation in postural tachycardia syndrome
Abstract
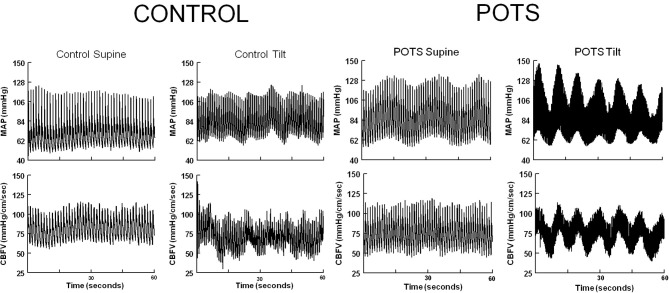
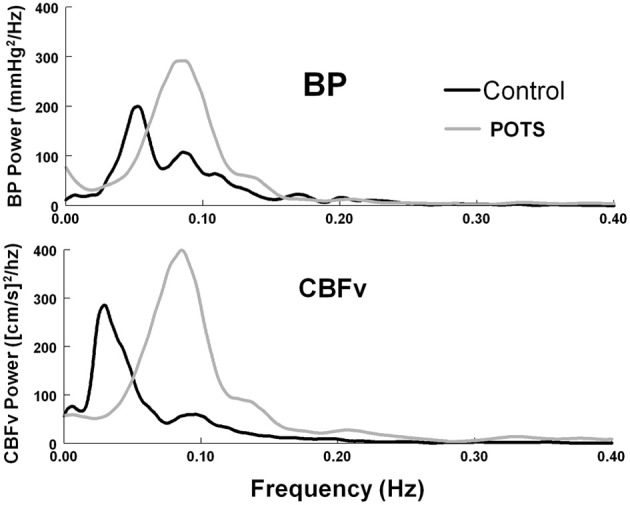
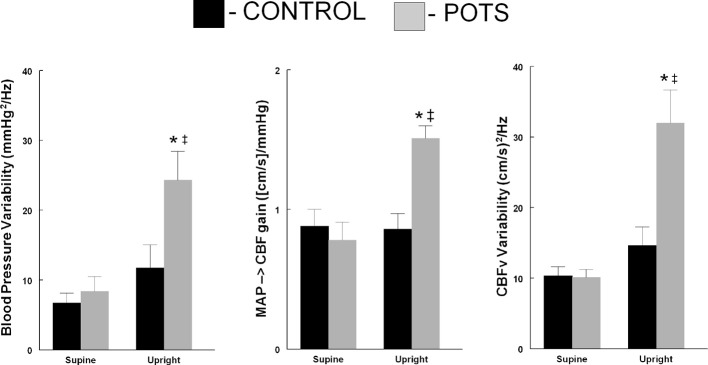
Decreased upright cerebral blood flow (CBF) with hyperpnea and hypocapnia is seen in a minority of patients with postural tachycardia syndrome (POTS). More often, CBF is not decreased despite upright neurocognitive dysfunction. This may result from time-dependent changes in CBF. We hypothesized that increased oscillations in CBF occurs in POTS (N = 12) compared to healthy controls (N = 9), and tested by measuring CBF velocity (CBFv) by transcranial Doppler ultrasound of the middle cerebral artery, mean arterial pressure (MAP) and related parameters, supine and during 70° upright tilt. Autospectra for mean CBFv and MAP, and transfer function analysis were obtained over the frequency range of 0.0078-0.4 Hz. Upright HR was increased in POTS (125 ± 8 vs. 86 ± 2 bpm), as was diastolic BP (74 ± 3 vs. 65 ± 3 mmHg) compared to control, while peripheral resistance, cardiac output, and mean CBFv increased similarly with tilt. Upright BP variability (BPV), low frequency (LF) power (0.04-0.13 Hz), and peak frequency of BPV were increased in POTS (24.3 ± 4.1, and 18.4 ± 4.1 mmHg(2)/Hz at 0.091 Hz vs. 11.8 ± 3.3, and 8.8 ± 2 mmHg(2)/Hz c at 0.071 Hz), as was upright overall CBFv variability, low frequency power and peak frequency of CBFv variability (29.3 ± 4.7, and 22.1 ± 2.7 [cm/s](2)/Hz at.092 Hz vs. 14.7 ± 2.6, and 6.7 ± 1.2 [cm/s](2)/Hz at 0.077Hz). Autospectra were sharply peaked in POTS. LF phase was decreased in POTS (-14 ± 4 vs. -25 ± 10 degrees) while upright. LF gain was increased (1.51 ± 0.09 vs. 0.86 ± 0.12 [cm/s]/ mmHg) while coherence was increased (0.96 ± 0.01 vs. 0.80 ± 0.04). Increased oscillatory BP in upright POTS patients is closely coupled to oscillatory CBFv over a narrow bandwidth corresponding to the Mayer wave frequency. Therefore combined increased oscillatory BP and increased LF gain markedly increases CBFv oscillations in a narrow bandwidth. This close coupling of CBF to MAP indicates impaired cerebral autoregulation that may underlie upright neurocognitive dysfunction in POTS.
Keywords: cerebral blood flow; mean arterial pressure autospectra; mean cerebral blood flow velocity autospectra; postural tachycardia syndrome; transfer function analysis; vasomotion.
Figures
Similar articles
-
Decreased upright cerebral blood flow and cerebral autoregulation in normocapnic postural tachycardia syndrome.Am J Physiol Heart Circ Physiol. 2009 Aug;297(2):H664-73. doi: 10.1152/ajpheart.00138.2009. Epub 2009 Jun 5. Am J Physiol Heart Circ Physiol. 2009. PMID: 19502561 Free PMC article.
-
Anticipatory central command on standing decreases cerebral blood velocity causing hypocapnia in hyperpneic postural tachycardia syndrome.J Appl Physiol (1985). 2023 Jul 1;135(1):26-34. doi: 10.1152/japplphysiol.00016.2023. Epub 2023 May 25. J Appl Physiol (1985). 2023. PMID: 37227184 Free PMC article.
-
Oscillatory cerebral blood flow is associated with impaired neurocognition and functional hyperemia in postural tachycardia syndrome during graded tilt.Hypertension. 2015 Mar;65(3):636-43. doi: 10.1161/HYPERTENSIONAHA.114.04576. Epub 2014 Dec 15. Hypertension. 2015. PMID: 25510829 Free PMC article.
-
Cerebral blood flow response to cardiorespiratory oscillations in healthy humans.Auton Neurosci. 2023 Mar;245:103069. doi: 10.1016/j.autneu.2022.103069. Epub 2022 Dec 23. Auton Neurosci. 2023. PMID: 36584666 Review.
-
Heart rate and heart rate variability comparison between postural orthostatic tachycardia syndrome versus healthy participants; a systematic review and meta-analysis.BMC Cardiovasc Disord. 2019 Dec 30;19(1):320. doi: 10.1186/s12872-019-01298-y. BMC Cardiovasc Disord. 2019. PMID: 31888497 Free PMC article.
Cited by
-
Postural tachycardia syndrome - Diagnosis, physiology, and prognosis.Auton Neurosci. 2018 Dec;215:3-11. doi: 10.1016/j.autneu.2018.02.005. Epub 2018 Feb 28. Auton Neurosci. 2018. PMID: 29523389 Free PMC article. Review.
-
Supine Parasympathetic Withdrawal and Upright Sympathetic Activation Underly Abnormalities of the Baroreflex in Postural Tachycardia Syndrome: Effects of Pyridostigmine and Digoxin.Hypertension. 2021 Apr;77(4):1234-1244. doi: 10.1161/HYPERTENSIONAHA.120.16113. Epub 2021 Jan 11. Hypertension. 2021. PMID: 33423527 Free PMC article.
-
Hypocapnic cerebral hypoperfusion: A biomarker of orthostatic intolerance.PLoS One. 2018 Sep 26;13(9):e0204419. doi: 10.1371/journal.pone.0204419. eCollection 2018. PLoS One. 2018. PMID: 30256820 Free PMC article.
-
Oscillatory lower body negative pressure impairs working memory task-related functional hyperemia in healthy volunteers.Am J Physiol Heart Circ Physiol. 2017 Apr 1;312(4):H672-H680. doi: 10.1152/ajpheart.00438.2016. Epub 2017 Feb 3. Am J Physiol Heart Circ Physiol. 2017. PMID: 28159806 Free PMC article.
-
Oscillatory lower body negative pressure impairs task related functional hyperemia in healthy volunteers.Am J Physiol Heart Circ Physiol. 2016 Mar 15;310(6):H775-84. doi: 10.1152/ajpheart.00747.2015. Epub 2016 Jan 22. Am J Physiol Heart Circ Physiol. 2016. PMID: 26801310 Free PMC article.
References
-
- Daubechies I. (1988). Orthonormal bases of compactly supported wavelets. Comm. Pure Appl. Math. 41, 909–996 10.1002/cpa.3160410705 - DOI
-
- Deegan B. M., Cooke J. P., Lyons D., Olaighin G., Serrador J. M. (2010). Cerebral autoregulation in the vertebral and middle cerebral arteries during combine head upright tilt and lower body negative pressure in healthy humans. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2010, 2505–2508 10.1109/IEMBS.2010.5626647 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources