

Variation and outcomes associated with direct hospital admission among children with pneumonia in the United States
- PMID: 25003562
- PMCID: PMC4529060
- DOI: 10.1001/jamapediatrics.2014.339
Variation and outcomes associated with direct hospital admission among children with pneumonia in the United States
Abstract
Importance: Although the majority of children with an unplanned admission to the hospital are admitted through the emergency department (ED), direct admissions constitute a significant proportion of hospital admissions nationally. Despite this, past studies of children have not characterized direct admission practices or outcomes. Pneumonia is the leading cause of pediatric hospitalization in the United States, providing an ideal lens to examine variation and outcomes associated with direct admissions.
Objectives: To describe rates and patterns of direct admission in a large sample of US hospitals and to compare resource utilization and outcomes between children with pneumonia admitted directly to a hospital and those admitted from an ED.
Design, setting, and participants: Retrospective cohort study of children 1 to 17 years of age with pneumonia who were admitted to hospitals contributing data to Perspective Data Warehouse. We developed hierarchical generalized linear models to examine associations between admission type and outcomes.
Main outcomes and measures: Outcome measures included (1) length of stay, (2) high turnover hospitalization, (3) total hospital cost, (4) transfer to the intensive care unit, and (5) readmission within 30 days of hospital discharge.
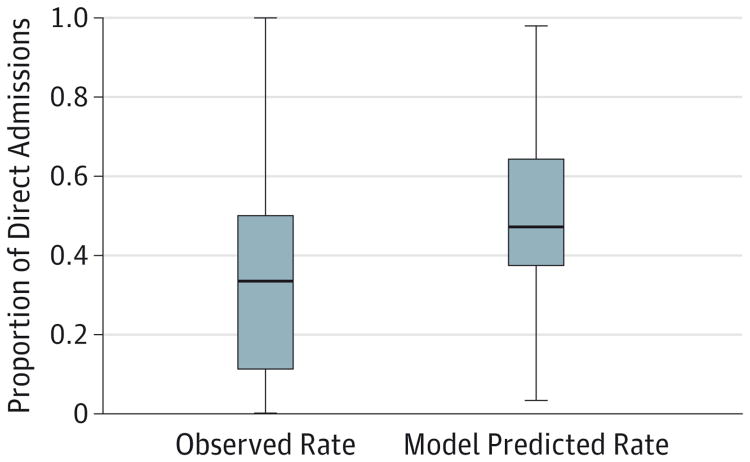
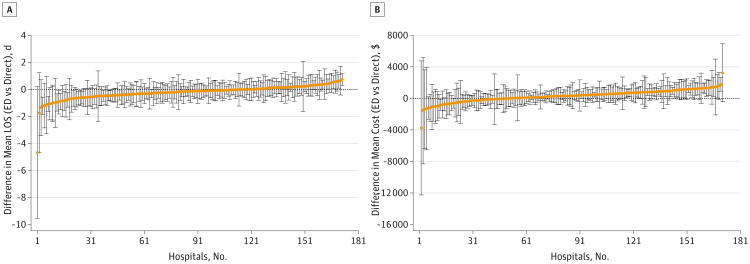
Results: A total of 19,736 children from 278 hospitals met eligibility criteria, including 7100 (36.0%) who were admitted directly and 12,636 (64.0%) through the ED. Rates of direct admission varied considerably across hospitals, with a median direct admission rate of 33.3% (interquartile range, 11.1%-50.0%). Children admitted directly were more likely to be white, to have private health insurance, and to be admitted to small, general community hospitals. In adjusted models, children admitted directly had a 9% higher length of stay (risk ratio, 1.09 [95% CI, 1.07-1.11]), 39% lower odds of high turnover hospitalization (odds ratio [OR], 0.61 [95% CI, 0.56-0.66]), and 12% lower cost (risk ratio, 0.88 [95% CI, 0.87-0.90]) than those admitted through the ED, with no significant differences in transfers to the intensive care unit (OR, 1.29 [95% CI, 0.83-2.00]) or 30-day readmissions (OR, 0.80 [95% CI, 0.57-1.13]).
Conclusions and relevance: Increasing rates of direct admission among children with access to outpatient care might be an effective strategy to reduce hospital costs and the volume of patients in the ED. Additional research is needed to establish direct admission policies and procedures that are safe and cost-effective.
Conflict of interest statement
Figures
References
-
- Committee on the Future of Emergency Care in the United States Health System; Board on Health Care Services; Institute of Medicine. Hospital-Based Emergency Care: At the Breaking Point. Washington, DC: National Academies Press; 2006.
-
- Merrill C, Owens PL. Reasons for being admitted to the hospital through the emergency department for children and adolescents, 2004. [Accessed February 10, 2014];Healthcare Cost and Utilization Project (HCUP) Statistical Brief 33. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb33.pdf. Published June 2007.
-
- Merrill C, Owens PL. Hospital admissions that began in the emergency department for children and adolescents, 2004. [Accessed February 10, 2014];Healthcare Costs and Utilization Project (HCUP) Statistical Brief 32. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb32.jsp. Published June 2007. - PubMed
-
- Kocher KE, Dimick JB, Nallamothu BK. Changes in the source of unscheduled hospitalizations in the United States. Med Care. 2013;51(8):689–698. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
