

Severe maternal sepsis in the UK, 2011-2012: a national case-control study
- PMID: 25003759
- PMCID: PMC4086731
- DOI: 10.1371/journal.pmed.1001672
Severe maternal sepsis in the UK, 2011-2012: a national case-control study
Abstract
Background: In light of increasing rates and severity of sepsis worldwide, this study aimed to estimate the incidence of, and describe the causative organisms, sources of infection, and risk factors for, severe maternal sepsis in the UK.
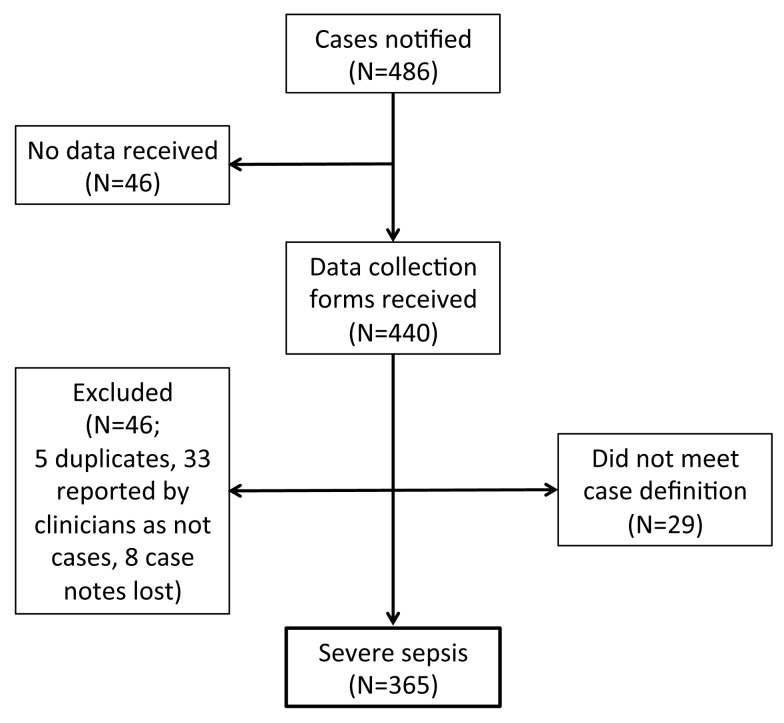
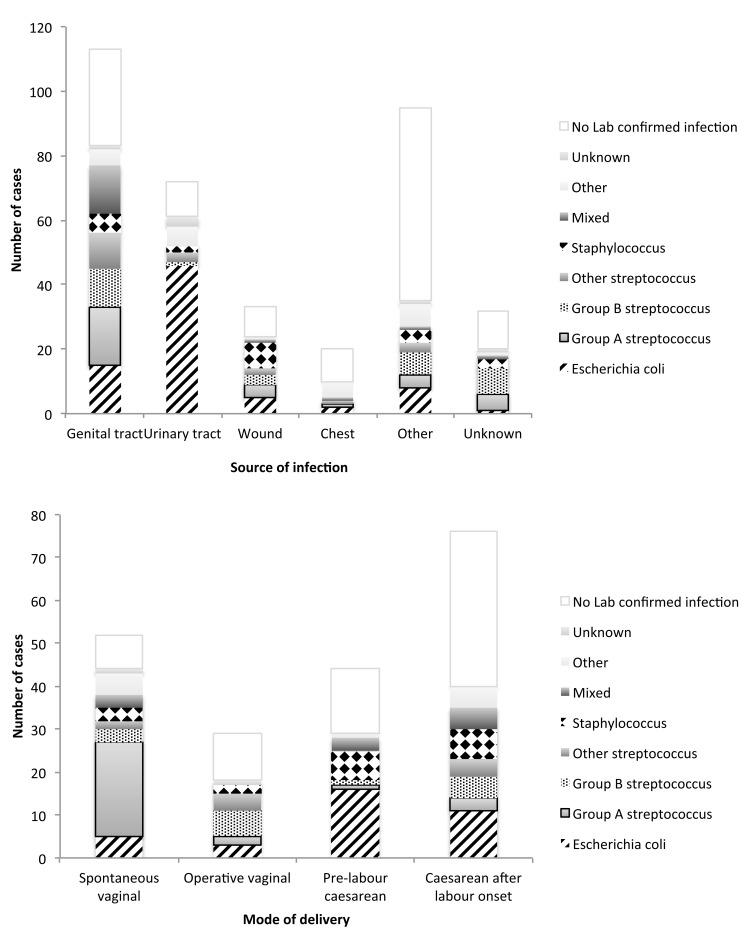
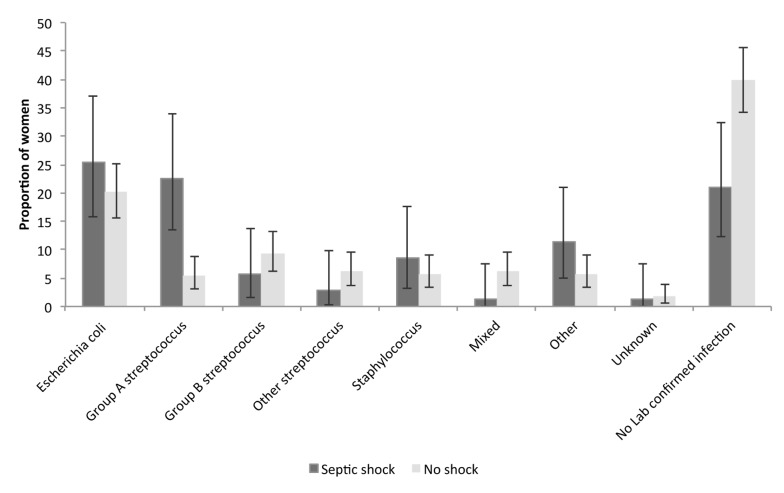
Methods and findings: A prospective case-control study included 365 confirmed cases of severe maternal sepsis and 757 controls from all UK obstetrician-led maternity units from June 1, 2011, to May 31, 2012. Incidence of severe sepsis was 4.7 (95% CI 4.2-5.2) per 10,000 maternities; 71 (19.5%) women developed septic shock; and five (1.4%) women died. Genital tract infection (31.0%) and the organism Escherichia coli (21.1%) were most common. Women had significantly increased adjusted odds ratios (aORs) of severe sepsis if they were black or other ethnic minority (aOR = 1.82; 95% CI 1.82-2.51), were primiparous (aOR = 1.60; 95% CI 1.17-2.20), had a pre-existing medical problem (aOR = 1.40; 95% CI 1.01-1.94), had febrile illness or were taking antibiotics in the 2 wk prior to presentation (aOR = 12.07; 95% CI 8.11-17.97), or had an operative vaginal delivery (aOR = 2.49; 95% CI 1.32-4.70), pre-labour cesarean (aOR = 3.83; 95% CI 2.24-6.56), or cesarean after labour onset (aOR = 8.06; 95% CI 4.65-13.97). Median time between delivery and sepsis was 3 d (interquartile range = 1-7 d). Multiple pregnancy (aOR = 5.75; 95% CI 1.54-21.45) and infection with group A streptococcus (aOR = 4.84; 2.17-10.78) were associated with progression to septic shock; for 16 (50%) women with a group A streptococcal infection there was <2 h-and for 24 (75%) women, <9 h-between the first sign of systemic inflammatory response syndrome and a diagnosis of severe sepsis. A limitation of this study was the proportion of women with sepsis without an identified organism or infection source (16.4%).
Conclusions: For each maternal sepsis death, approximately 50 women have life-threatening morbidity from sepsis. Follow-up to ensure infection is eradicated is important. The rapid progression to severe sepsis highlights the importance of following the international Surviving Sepsis Campaign guideline of early administration of high-dose intravenous antibiotics within 1 h of admission to hospital for anyone with suspected sepsis. Signs of severe sepsis in peripartum women, particularly with confirmed or suspected group A streptococcal infection, should be regarded as an obstetric emergency. Please see later in the article for the Editors' Summary.
Conflict of interest statement
SS is Chair of the Claims Advisory Committee at the Medical Protection Society for which she receives an honorarium. All other authors have declared that no competing interests exist.
Figures
References
-
- Cantwell R, Clutton-Brock T, Cooper G, Dawson A, Drife J, et al. (2011) Saving mothers' lives: reviewing maternal deaths to make motherhood safer: 2006–2008. The eighth report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG 118 (Suppl 1) 1–203 10.1111/j.1471-0528.2010.02847.x - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
