

Effect of home visiting by nurses on maternal and child mortality: results of a 2-decade follow-up of a randomized clinical trial
- PMID: 25003802
- PMCID: PMC4235164
- DOI: 10.1001/jamapediatrics.2014.472
Effect of home visiting by nurses on maternal and child mortality: results of a 2-decade follow-up of a randomized clinical trial
Abstract
Importance: Mothers and children living in adverse contexts are at risk of premature death.
Objective: To determine the effect of prenatal and infant/toddler nurse home visiting on maternal and child mortality during a 2-decade period (1990-2011).
Design, setting, and participants: A randomized clinical trial was designed originally to assess the home visiting program's effect on pregnancy outcomes and maternal and child health through child age 2 years. The study was conducted in a public system of obstetric and pediatric care in Memphis, Tennessee. Participants included primarily African American women and their first live-born children living in highly disadvantaged urban neighborhoods, who were assigned to 1 of 4 treatment groups: treatment 1 (transportation for prenatal care [n = 166]), treatment 2 (transportation plus developmental screening for infants and toddlers [n = 514]), treatment 3 (transportation plus prenatal/postpartum home visiting [n = 230]), and treatment 4 (transportation, screening, and prenatal, postpartum, and infant/toddler home visiting [n = 228]). Treatments 1 and 3 were included originally to increase statistical power for testing pregnancy outcomes. For determining mortality, background information was available for all 1138 mothers assigned to all 4 treatments and all but 2 live-born children in treatments 2 and 4 (n = 704). Inclusion of children in treatments 1 and 3 was not possible because background information was missing on too many children.
Interventions: Nurses sought to improve the outcomes of pregnancy, children's health and development, and mothers' health and life-course with home visits beginning during pregnancy and continuing through child age 2 years.
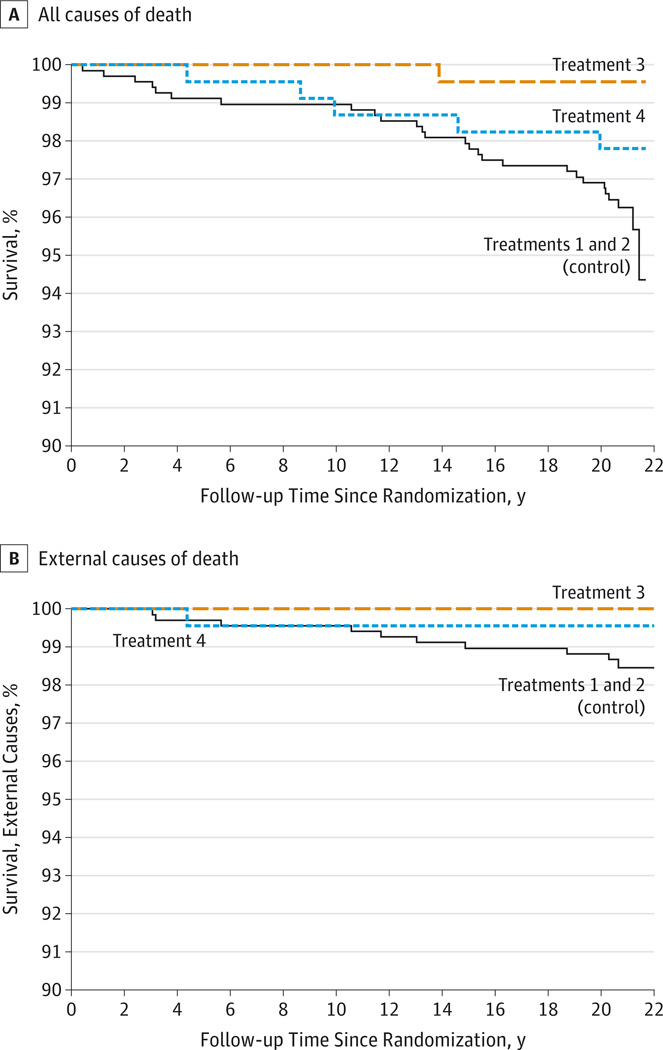
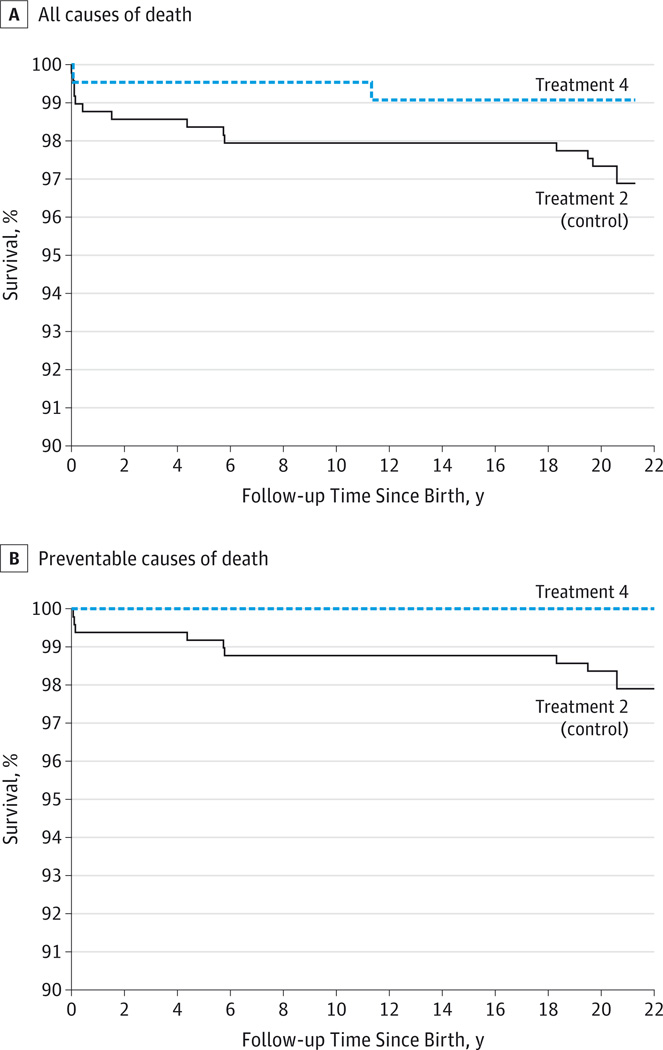
Main outcomes and measures: All-cause mortality in mothers and preventable-cause mortality in children (sudden infant death syndrome, unintentional injury, and homicide) derived from the National Death Index.
Results: The mean (SE) 21-year maternal all-cause mortality rate was 3.7% (0.74%) in the combined control group (treatments 1 and 2), 0.4% (0.43%) in treatment 3, and 2.2% (0.97%) in treatment 4. The survival contrast of treatments 1 and 2 combined with treatment 3 was significant (P = .007); the contrast of treatments 1 and 2 combined with treatment 4 was not significant (P = .19), and the contrast of treatments 1 and 2 combined with treatments 3 and 4 combined was significant (post hoc P = .008). At child age 20 years, the preventable-cause child mortality rate was 1.6% (0.57%) in treatment 2 and 0.0% (SE not calculable) in treatment 4; the survival contrast was significant (P = .04).
Conclusions and relevance: Prenatal and infant/toddler home visitation by nurses is a promising means of reducing all-cause mortality among mothers and preventable-cause mortality in their first-born children living in highly disadvantaged settings.
Trial registration: clinicaltrials.gov Identifier: NCT00708695.
Conflict of interest statement
Figures
References
-
- Murphy SL, Xu J, Kochabek KD. National Vital Statistics Reports. Deaths: final data for 2010. [Accessed May 23, 2014];National Vital Statistics Systems. 2013 61(4) http://www.cdc.gov/nchs/data/nvsr/nvsr61/nvsr61_04.pdf. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
