

The use of novel drugs can effectively improve response, delay relapse and enhance overall survival in multiple myeloma patients with renal impairment
- PMID: 25003848
- PMCID: PMC4086950
- DOI: 10.1371/journal.pone.0101819
The use of novel drugs can effectively improve response, delay relapse and enhance overall survival in multiple myeloma patients with renal impairment
Abstract
Background: Renal impairment is a common feature in multiple myeloma and is considered a poor prognostic factor.
Aim: To determine the impact of novel drugs (i.e. bortezomib, lenalidomide and thalidomide) in the treatment of myeloma patients with renal impairment. The primary endpoint was overall survival and secondary endpoints were time to next treatment and response.
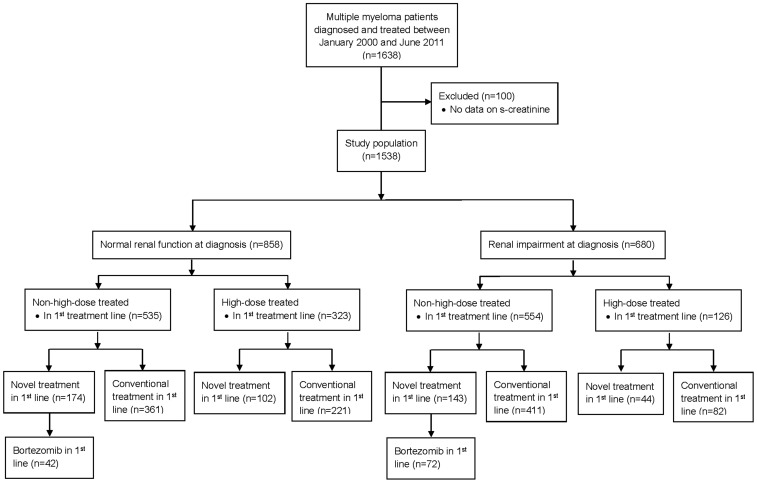
Methods: The study population included all patients diagnosed with treatment-demanding multiple myeloma January 2000 to June 2011 at 15 Swedish hospitals. Renal impairment was defined as an estimated glomerular filtration rate under 60 mL/min/1.73 m2.
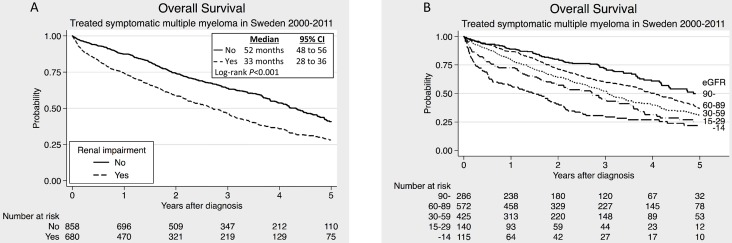
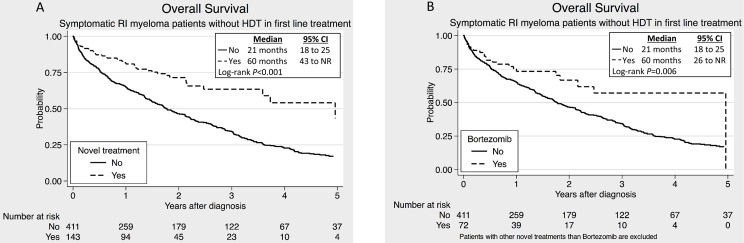
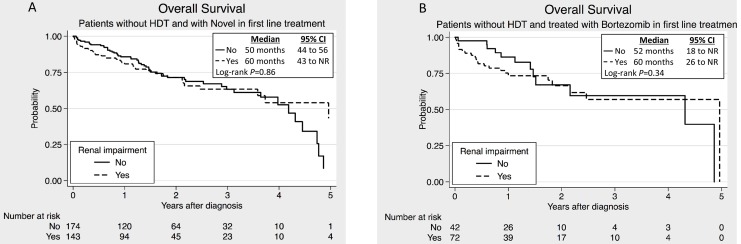
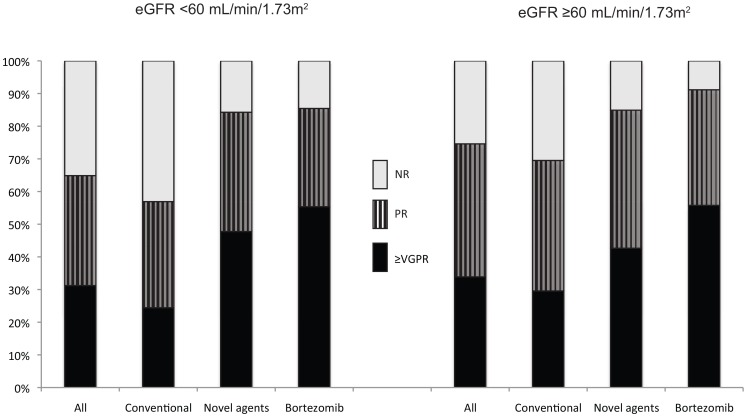
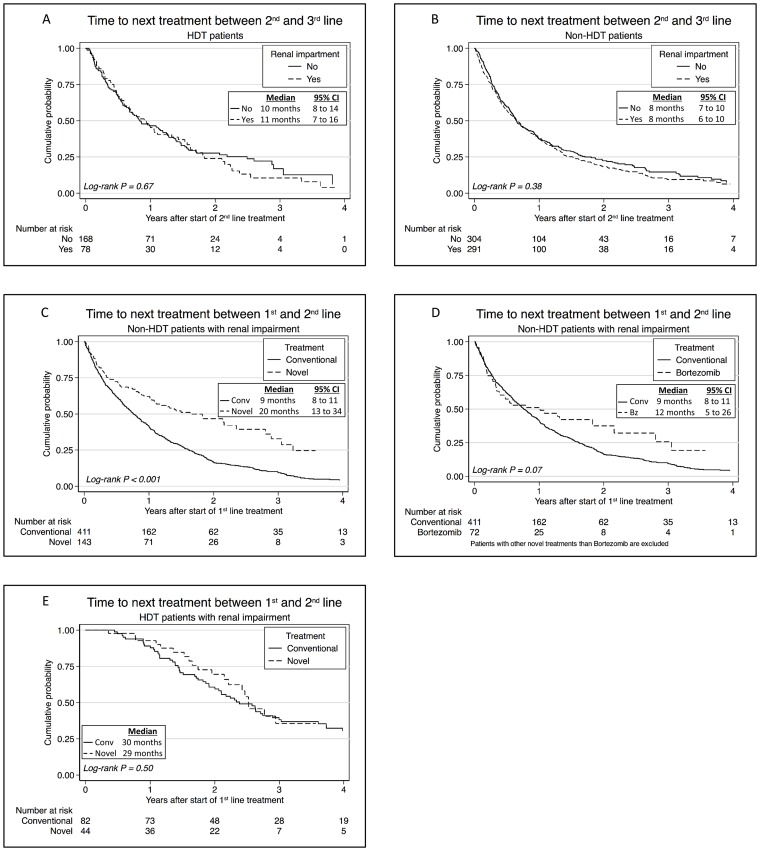
Result: The study population consisted of 1538 patients, of which 680 had renal impairment at diagnosis. The median overall survival in patients with renal impairment was 33 months, which was significantly shorter than 52 months in patients with normal renal function (P<0.001). Novel agents in first line improved overall survival (median 60 months) in non-high-dose treated patients with renal impairment (n = 143) as compared to those treated with conventional cytotoxic drugs (n = 411) (median 27 months) (P<0.001). In the multivariate analysis up front treatment with bortezomib was an independent factor for better overall survival in non-high-dose treated renally impaired patients. High-dose treated renally impaired patients had significantly better median overall survival than non-high-dose ones (74 versus 26 months) and novel drugs did not significantly improve survival further in these patients. Patients with renal impairment had both a shorter median time to next treatment and a lower response rate than those with normal renal function. However, novel drugs and high dose treatment lead to a significantly longer time to next treatment and the use of novel agents significantly improved the response rate of these patients.
Conclusion: High dose treatment and novel drugs, especially bortezomib, can effectively overcome the negative impact of renal impairment in patients with multiple myeloma.
Conflict of interest statement
Figures
References
-
- Chanan-Khan AA, Giralt S (2010) Importance of achieving a complete response in multiple myeloma, and the impact of novel agents. J Clin Oncol 28: 2612–2624. - PubMed
-
- Dingli D, Pacheco JM, Nowakowski GS, Kumar SK, Dispenzieri A, et al. (2007) Relationship between depth of response and outcome in multiple myeloma. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 25: 4933–4937. - PubMed
-
- Alexanian R, Barlogie B, Dixon D (1990) Renal failure in multiple myeloma. Pathogenesis and prognostic implications. Archives of internal medicine 150: 1693–1695. - PubMed
-
- Abbott KC, Agodoa LY (2001) Multiple myeloma and light chain-associated nephropathy at end-stage renal disease in the United States: patient characteristics and survival. Clinical nephrology 56: 207–210. - PubMed
-
- Rayner HC, Haynes AP, Thompson JR, Russell N, Fletcher J (1991) Perspectives in multiple myeloma: survival, prognostic factors and disease complications in a single centre between 1975 and 1988. The Quarterly journal of medicine 79: 517–525. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
