

Management of variceal hemorrhage: current concepts
- PMID: 25004293
- PMCID: PMC4678684
- DOI: 10.1590/s0102-67202014000200011
Management of variceal hemorrhage: current concepts
Abstract
Introduction: The treatment of portal hypertension is complex and the the best strategy depends on the underlying disease (cirrhosis vs. schistosomiasis), patient's clinical condition and time on it is performed (during an acute episode of variceal bleeding or electively, as pre-primary, primary or secondary prophylaxis). With the advent of new pharmacological options and technical development of endoscopy and interventional radiology treatment of portal hypertension has changed in recent decades.
Aim: To review the strategies employed in elective and emergency treatment of variceal bleeding in cirrhotic and schistosomotic patients.
Methods: Survey of publications in PubMed, Embase, Lilacs, SciELO and Cochrane databases through June 2013, using the headings: portal hypertension, esophageal and gastric varices, variceal bleeding, liver cirrhosis, schistosomiasis mansoni, surgical treatment, pharmacological treatment, secondary prophylaxis, primary prophylaxis, pre-primary prophylaxis.
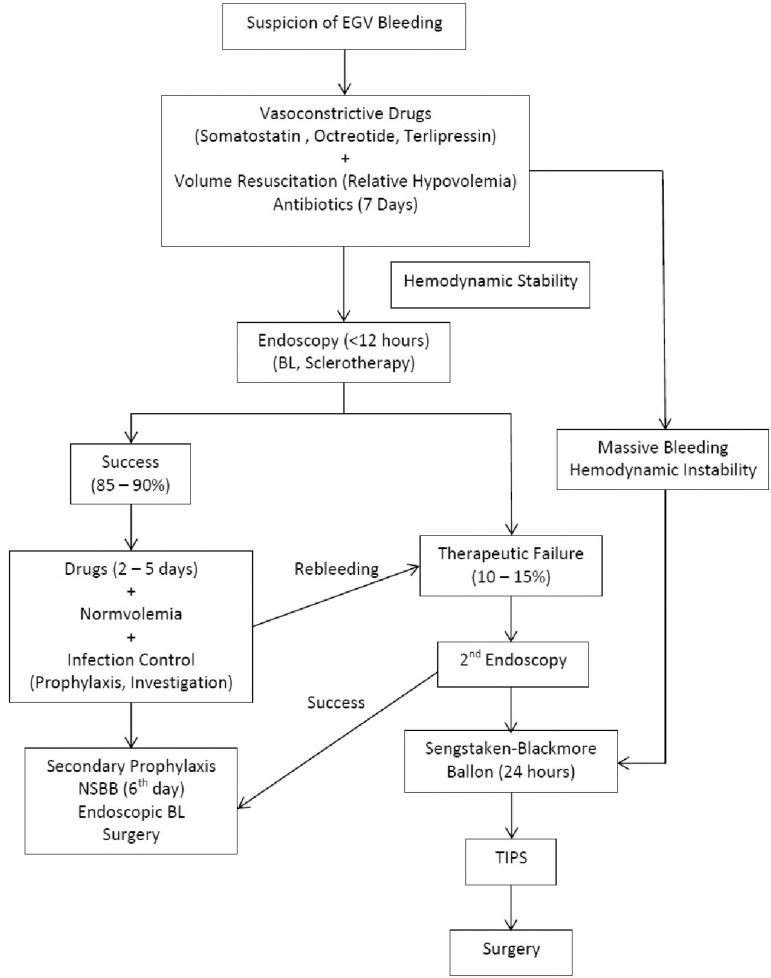
Conclusion: Pre-primary prophylaxis doesn't have specific treatment strategies; the best recommendation is treatment of the underlying disease. Primary prophylaxis should be performed in cirrhotic patients with beta-blockers or endoscopic variceal ligation. There is controversy regarding the effectiveness of primary prophylaxis in patients with schistosomiasis; when indicated, it is done with beta-blockers or endoscopic therapy in high-risk varices. Treatment of acute variceal bleeding is systematized in the literature, combination of vasoconstrictor drugs and endoscopic therapy, provided significant decline in mortality over the last decades. TIPS and surgical treatment are options as rescue therapy. Secondary prophylaxis plays a fundamental role in the reduction of recurrent bleeding, the best option in cirrhotic patients is the combination of pharmacological therapy with beta-blockers and endoscopic band ligation. TIPS or surgical treatment, are options for controlling rebleeding on failure of secondary prophylaxis. Despite the increasing evidence of the effectiveness of pharmacological and endoscopic treatment in schistosomotic patients, surgical therapy still plays an important role in secondary prophylaxis.
Introdução: O tratamento da hipertensão portal é complexo e a definição da melhor estratégia depende da causa subjacente (cirrose vs. Esquistossomose), da condição clínica e do momento em que é realizado (episódio agudo de hemorragia ou como profilaxia pré-primária, primária ou secundária). Com o advento de novas opções medicamentosas e o desenvolvimento da endoscopia e radiologia intervencionista, o tratamento da hipertensão portal tem sofrido grande transformação nas últimas décadas.
Objetivo: Avaliar os avanços e as estratégias empregadas no tratamento emergencial e eletivo da hemorragia varicosa em pacientes cirróticos e esquistossomóticos.
Método: Revisão bibliográfica nas bases de dados PubMed, Embase, Lilacs, SciELO e Cochrane até junho de 2013, com os descritores: portal hypertension, esophageal and gastric varices, variceal bleeding, liver cirrhosis, schistosomiasis mansoni, surgical treatment, pharmacological treatment, secondary prophylaxis, primary prophylaxis, pré-primary prophylaxis.
Conclusão: Com relação à profilaxia pré-primária não existem estratégias específicas; a melhor recomendação é tratamento da doença de base. A proflaxia primária em pacientes cirróticos deve ser feita com betabloqueadores ou terapêutica endoscópica com ligadura elástica. Existe controvérsia quanto à efetividade da profilaxia primária em pacientes esquistossomóticos; quando indicada, faz-se com betabloqueadores ou terapêutica endoscópica nas varizes de maior risco. O tratamento do sangramento agudo é o com melhor sistematização e mais alto nível de evidência; a associação de drogas vasoconstritoras e terapia endoscópica proporcionou queda significativa na mortalidade nas últimas décadas. O TIPS e o tratamento cirúrgico são opções na terapia de resgate. A profilaxia secundária é feita com terapia farmacológica (betabloqueadores) e endoscópica em pacientes cirróticos. Na falha da profilaxia secundária, o TIPS ou o tratamento cirúrgico são opções viáveis para controle da recidiva hemorrágica. Apesar do aumento das evidências da eficácia da terapêutica farmacológica e endoscópica em pacientes esquistossomóticos, o tratamento cirúrgico ainda tem papel preponderante na profilaxia secundária destes pacientes.
Conflict of interest statement
Conflicts of interest: none
Figures
Similar articles
-
Endoscopic diagnosis and management of esophagogastric variceal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline.Endoscopy. 2022 Nov;54(11):1094-1120. doi: 10.1055/a-1939-4887. Epub 2022 Sep 29. Endoscopy. 2022. PMID: 36174643
-
[Variceal upper digestive bleeding--an ever new complication in liver cirrhosis].Rev Med Chir Soc Med Nat Iasi. 2007 Jan-Mar;111(1):19-26. Rev Med Chir Soc Med Nat Iasi. 2007. PMID: 17595842 Review. Romanian.
-
Role of band ligation for secondary prophylaxis of variceal bleeding.World J Gastroenterol. 2018 Jul 14;24(26):2902-2914. doi: 10.3748/wjg.v24.i26.2902. World J Gastroenterol. 2018. PMID: 30018485 Free PMC article.
-
Partial splenic embolization as a rescue and emergency treatment for portal hypertension and gastroesophageal variceal hemorrhage.BMC Gastroenterol. 2023 May 24;23(1):180. doi: 10.1186/s12876-023-02808-1. BMC Gastroenterol. 2023. PMID: 37226088 Free PMC article.
-
Band ligation versus sham or no intervention for primary prophylaxis of oesophageal variceal bleeding in children and adolescents with chronic liver disease or portal vein thrombosis.Cochrane Database Syst Rev. 2021 Jan 26;1(1):CD011561. doi: 10.1002/14651858.CD011561.pub2. Cochrane Database Syst Rev. 2021. PMID: 33522602 Free PMC article.
Cited by
-
Risk stratification in acute variceal bleeding: Far from an ideal score.Clinics (Sao Paulo). 2021 Jun 28;76:e2921. doi: 10.6061/clinics/2021/e2921. eCollection 2021. Clinics (Sao Paulo). 2021. PMID: 34190855 Free PMC article.
-
Educational Case: Evaluating a patient with cirrhosis.Acad Pathol. 2022 Jul 1;9(1):100031. doi: 10.1016/j.acpath.2022.100031. eCollection 2022. Acad Pathol. 2022. PMID: 35813091 Free PMC article. No abstract available.
-
Effects of Transjugular Intrahepatic Portosystemic Shunt on Renal and Pulmonary Function in Hepatic Decompensation with and without Hepatorenal and Hepatopulmonary Syndromes: A Review.J Clin Transl Hepatol. 2024 Sep 28;12(9):780-791. doi: 10.14218/JCTH.2024.00188. Epub 2024 Jul 25. J Clin Transl Hepatol. 2024. PMID: 39280072 Free PMC article. Review.
-
Anemia in cirrhosis: An underestimated entity.World J Clin Cases. 2022 Jan 21;10(3):777-789. doi: 10.12998/wjcc.v10.i3.777. World J Clin Cases. 2022. PMID: 35127894 Free PMC article. Review.
-
Morbidity and Mortality Due to Schistosoma mansoni Related Periportal Fibrosis: Could Early Diagnosis of Varices Improve the Outcome Following Available Treatment Modalities in Sub Saharan Africa? A Scoping Review.Trop Med Infect Dis. 2020 Feb 3;5(1):20. doi: 10.3390/tropicalmed5010020. Trop Med Infect Dis. 2020. PMID: 32028581 Free PMC article.
References
-
- Bernard B, Lebrec D, Mathurin P, Opolon P, Poynard T. Betaadrenergic antagonists in the prevention of gastrointestinal rebleeding in patients with cirrhosis: a meta-analysis. Hepatology. 1997;25:63–67. - PubMed
-
- Bittencourt PL, Farias AQ, Strauss E, Mattos AA. Panel of the 1st Brazilian Consensus of Variceal Bleeding, Brazilian Society of Hepatology. Variceal bleeding: consensus meeting report from the Brazilian Society of Hepatology. Arq Gastroenterol. 2010;47(2):202–216. - PubMed
-
- Capussotti L, Vergara V, Polastri R, Bouzari H, Galatola G. Liver function and encephalopathy after partial vs direct side-to-side portacaval shunt: a prospective randomized clinical trial. Surgery. 2000;127(6):614–621. - PubMed
-
- Carbonell N, Pauwels A, Serfaty L, Fourdan O, Lévy VG, Poupon R. Improved survival after variceal bleeding in patients with cirrhosis over the past two decades. Hepatology. 2004;40:652–659. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
