

Femoral versus radial access in primary angioplasty. Analysis of the ACCEPT registry
- PMID: 25004418
- PMCID: PMC4079020
- DOI: 10.5935/abc.20140063
Femoral versus radial access in primary angioplasty. Analysis of the ACCEPT registry
Abstract
Background: The radial access provides a lower risk of bleeding and vascular complications related to the puncture site in comparison to the femoral access. Recent studies have suggested a reduction in mortality associated with the radial access in patients with acute myocardial infarction undergoing percutaneous coronary intervention.
Objective: To compare the occurrence of adverse cardiovascular ischemic and hemorrhagic events in patients undergoing primary angioplasty according to the type of arterial access route.
Methods: From August 2010 to December 2011, 588 patients undergoing primary percutaneous coronary intervention during acute ST-segment elevation myocardial infarction were assessed; they were recruited from 47 centers participating in the ACCEPT registry. Patients were grouped and compared according to the arterial access used for the procedure.
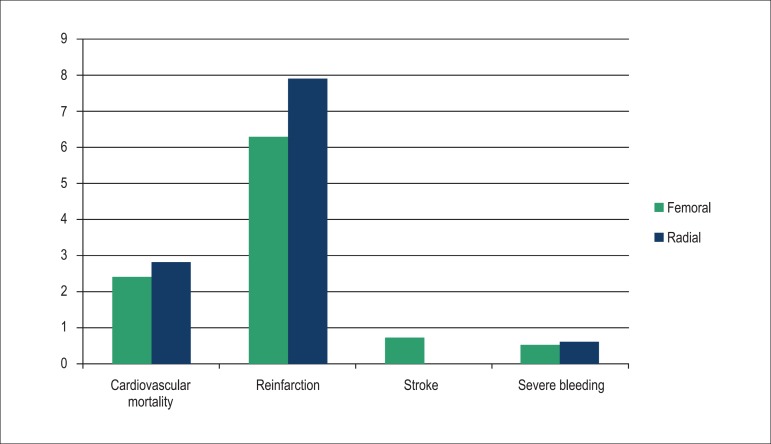
Results: The mean age was 61.8 years; 75% were males and 24% had diabetes mellitus. There was no difference between groups as regards the procedure success rate, as well as regards the occurrence of death, reinfarction, or stroke at six months of follow-up. Severe bleeding was reported in 1.1% of the sample analyzed, with no statistical difference related to the access used.
Conclusions: The femoral and radial accesses are equally safe and effective for the performance of primary percutaneous coronary intervention. The low rate of cardiovascular events and of hemorrhagic complications reflects the quality of the participating centers and the operators expertise with the use of both techniques.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Pocock SJ, Mehran R, Clayton TC, Nikolsky E, Parise H, Fahy M, et al. Prognostic modeling of individual patient risk and mortality impact of ischemic and hemorrhagic complications: assessment from the Acute Catheterization and Urgent Intervention Triage Strategy trial. Circulation. 2010;121(1):43–51. - PubMed
-
- Doyle BJ, Rihal CS, Gastineau DA, Holmes, Jr DR. Bleeding, blood transfusion, and increased mortality after percutaneous coronary intervention: implications for contemporary practice. J Am Coll Cardiol Interv. 2009;22(22):2019–2027. - PubMed
-
- de Andrade PB, Tebet MA, Maia da Silva FS, Athanazio de Andrade MV, Labrunie A, Piva e Mattos LA. Major bleeding in acute coronary syndromes. J Invasive Cardiol. 2011;23(11):485–490. - PubMed
-
- Ndrepepa G, Neumann FJ, Richardt G, Schulz S, Tölg R, Stoyanov KM, et al. Prognostic value of access and non-access sites bleeding after percutaneous coronary intervention. Circ Cardiovasc Interv. 2013;6(4):354–361. - PubMed
-
- Steg PG, James SK, Atar D, Badano LP, Blomstrom-Lundqvist C, Borger MA, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force on the management of St-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC) Eur Heart J. 2012;33(20):2569–2619. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
