

Baroreflex sensitivity and its association with arrhythmic events in Chagas disease
- PMID: 25004420
- PMCID: PMC4079022
- DOI: 10.5935/abc.20140066
Baroreflex sensitivity and its association with arrhythmic events in Chagas disease
Abstract
Background: Sudden death is the leading cause of death in Chagas disease (CD), even in patients with preserved ejection fraction (EF), suggesting that destabilizing factors of the arrhythmogenic substrate (autonomic modulation) contribute to its occurrence.
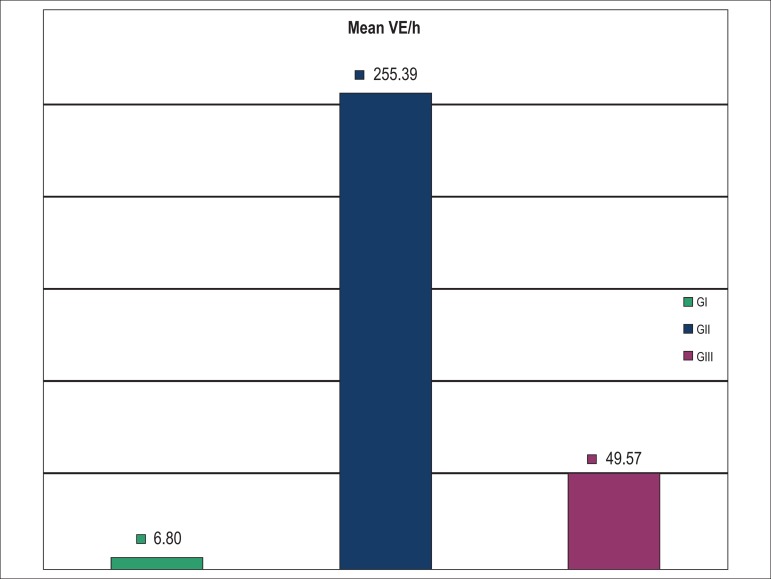
Objective: To determine baroreflex sensitivity (BRS) in patients with undetermined CD (GI), arrhythmogenic CD with nonsustained ventricular tachycardia (NSVT) (GII) and CD with spontaneous sustained ventricular tachycardia (STV) (GIII), to evaluate its association with the occurrence and complexity of arrhythmias.
Method: Forty-two patients with CD underwent ECG and continuous and noninvasive BP monitoring (TASK force monitor). The following were determined: BRS (phenylephrine method); heart rate variability (HRV) on 24-h Holter; and EF (echocardiogram).
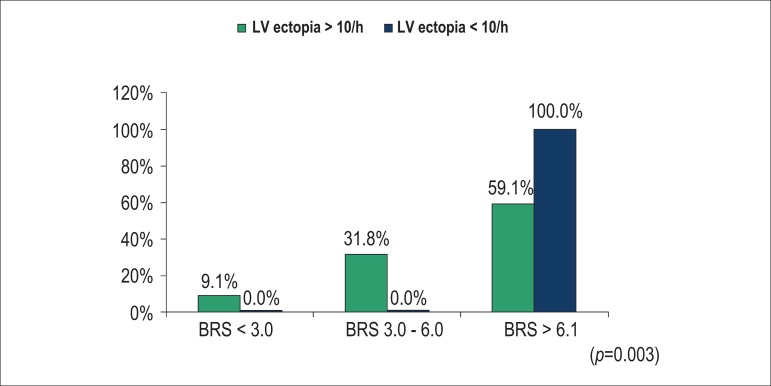
Results: GIII had lower BRS (6.09 ms/mm Hg) as compared to GII (11.84) and GI (15.23). The difference was significant between GI and GIII (p = 0.01). Correlating BRS with the density of ventricular extrasystoles (VE), low VE density (<10/h) was associated with preserved BRS. Only 59% of the patients with high VE density (> 10/h) had preserved BRS (p = 0.003). Patients with depressed BRS had higher VE density (p = 0.01), regardless of the EF. The BRS was the only variable related to the occurrence of SVT (p = 0.028).
Conclusion: The BRS is preserved in undetermined CD. The BRS impairment increases as disease progresses, being more severe in patients with more complex ventricular arrhythmias. The degree of autonomic dysfunction did not correlate with EF, but with the density and complexity of ventricular arrhythmias.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Rassi Jr A, Rassi AG, Rassi SG, Rassi Jr L, Rassi A. Relação entre sintomas, disfunção ventricular e arritmia ventricular na cardiopatia chagásica crônica. Arq Bras Cardiol. 1992;59(supl 2):182–182.
-
- Rassi A. Curva atuarial da taquicardia ventricular sustentada na cardiopatia chagásica crônica; Anais do IV Simpósio Brasileiro de Arritmias Cardíacas; Recife. 1987.
-
- Prata A. Clinical and epidemiological aspects of Chagas disease. Lancet Infec Dis. 2001;1(2):92–100. - PubMed
-
- Lopes ER, Chapadeiro E. Morte súbita em área endêmica da doença de Chagas. Rev Soc Bras Med Trop. 1982;16(2):79–84.
-
- Dias E, Laranja FS, Miranda A, Nobrega G. Chagas' disease: a clinical, epidemiologic and pathologic study. Circulation. 1956;14(6):1035–1060. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
