

Hospital level under-utilization of minimally invasive surgery in the United States: retrospective review
- PMID: 25005264
- PMCID: PMC4087169
- DOI: 10.1136/bmj.g4198
Hospital level under-utilization of minimally invasive surgery in the United States: retrospective review
Abstract
Objective: To determine casemix adjusted hospital level utilization of minimally invasive surgery for four common surgical procedures (appendectomy, colectomy, total abdominal hysterectomy, and lung lobectomy) in the United States.
Design: Retrospective review.
Setting: United States.
Participants: Nationwide inpatient sample database, United States 2010.
Methods: For each procedure, a propensity score model was used to calculate the predicted proportion of minimally invasive operations for each hospital based on patient characteristics. For each procedure, hospitals were categorized into thirds (low, medium, and high) based on their actual to predicted proportion of utilization of minimally invasive surgery.
Main outcome measures: The primary outcome measures were the actual and predicted proportion of procedures performed with minimally invasive surgery. Secondary outcome measures included surgical complications and hospital characteristics.
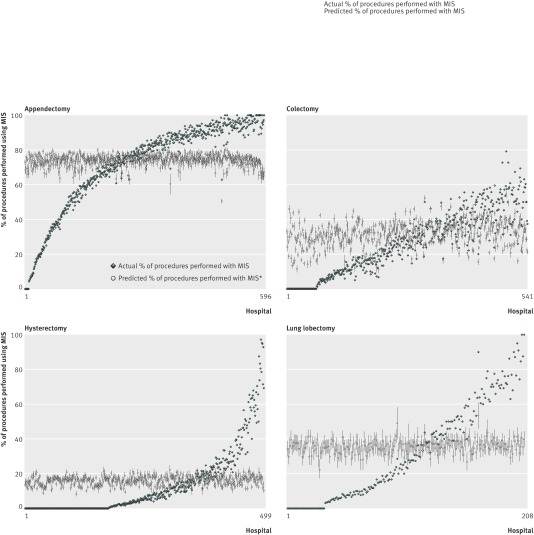
Results: Mean hospital utilization of minimally invasive surgery was 71.0% (423/596) for appendectomy (range 40.9-93.1% (244-555)), 28.4% (154/541) for colectomy (6.7-49.8% (36/541-269/541)), 13.0% (65/499) for hysterectomy (0.0-33.6% (0/499-168/499)), and 32.0% (67/208) for lung lobectomy (3.6-65.7% (7.5/208-137/208)). Utilization of minimally invasive surgery was highly variable for each procedure type. There was noticeable discordance between actual and predicted utilization of the surgery (range of actual to predicted ratio for appendectomy 0-1.49; colectomy 0-3.88; hysterectomy 0-6.68; lung lobectomy 0-2.51). Surgical complications were less common with minimally invasive surgery compared with open surgery, respectively: overall rate for appendectomy 3.94% (1439/36,513) v 7.90% (958/12,123), P<0.001; for colectomy: 13.8% (1689/12,242) v 35.8% (8837/24,687), P<0.001; for hysterectomy: 4.69% (270/5757) v 6.64% (1988/29,940), P<0.001; and for lung lobectomy: 17.1% (367/2145) v 25.4% (971/3824), P<0.05. High utilization of minimally invasive surgery was associated with urban location (appendectomy: odds ratio 4.66, 95% confidence interval 1.17 to 18.5; colectomy: 4.59, 1.04 to 20.3; hysterectomy: 15.0, 2.98 to 75.0), large hospital size (hysterectomy: 8.70, 1.62 to 46.8), teaching hospital (hysterectomy: 5.41, 1.27 to 23.1), Midwest region (appendectomy: 7.85, 1.26 to 49.1), south region (appendectomy: 21.0, 3.79 to 117; colectomy: 10.0, 1.83 to 54.7), and west region (appendectomy: 9.33, 1.48 to 58.8).
Conclusion: Hospital utilization of minimally invasive surgery for appendectomy, colectomy, total abdominal hysterectomy, and lung lobectomy varies widely in the United States, representing a disparity in the surgical care delivered nationwide.
© Cooper et al 2014.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Mangano DT. Perioperative medicine: NHLBI working group deliberations and recommendations. J Cardiothorac Vasc Anesth 2004;18:1-6. - PubMed
-
- Sauerland S, Jaschinski T, Neugebauer EA. Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database Syst Rev 2010;10:CD001546. - PubMed
-
- Clinical Outcomes of Surgical Therapy Study Group. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 2004;350:2050-9. - PubMed
-
- Nieboer TE, Johnson N, Lethaby A, Tavender E, Curr E, Garry R, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev 2009;3:CD003677.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical