

A comparison of different diagnostic criteria of acute kidney injury in critically ill patients
- PMID: 25005361
- PMCID: PMC4227114
- DOI: 10.1186/cc13977
A comparison of different diagnostic criteria of acute kidney injury in critically ill patients
Abstract
Introduction: Recently, the Kidney Disease: Improving Global Outcomes (KDIGO) proposed a new definition and classification of acute kidney injury (AKI) on the basis of the RIFLE (Risk, Injury, Failure, Loss of kidney function, and End-stage renal failure) and AKIN (Acute Kidney Injury Network) criteria, but comparisons of the three criteria in critically ill patients are rare.
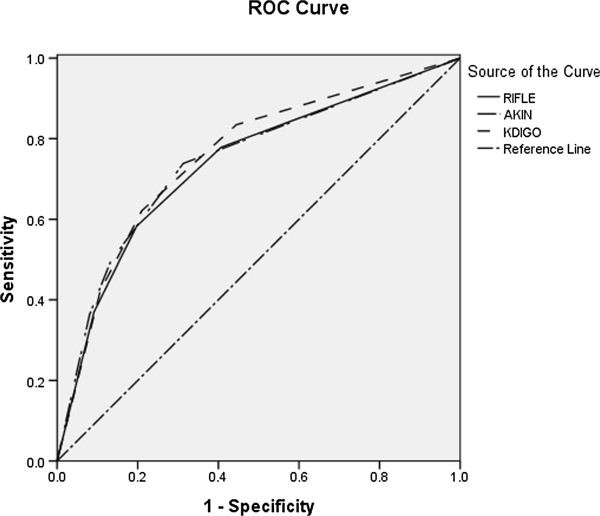
Methods: We prospectively analyzed a clinical database of 3,107 adult patients who were consecutively admitted to one of 30 intensive care units of 28 tertiary hospitals in Beijing from 1 March to 31 August 2012. AKI was defined by the RIFLE, AKIN, and KDIGO criteria. Receiver operating curves were used to compare the predictive ability for mortality, and logistic regression analysis was used for the calculation of odds ratios and 95% confidence intervals.
Results: The rates of incidence of AKI using the RIFLE, AKIN, and KDIGO criteria were 46.9%, 38.4%, and 51%, respectively. KDIGO identified more patients than did RIFLE (51% versus 46.9%, P = 0.001) and AKIN (51% versus 38.4%, P <0.001). Compared with patients without AKI, in-hospital mortality was significantly higher for those diagnosed as AKI by using the RIFLE (27.8% versus 7%, P <0.001), AKIN (32.2% versus 7.1%, P <0.001), and KDIGO (27.4% versus 5.6%, P <0.001) criteria, respectively. There was no difference in AKI-related mortality between RIFLE and KDIGO (27.8% versus 27.4%, P = 0.815), but there was significant difference between AKIN and KDIGO (32.2% versus 27.4%, P = 0.006). The areas under the receiver operator characteristic curve for in-hospital mortality were 0.738 (P <0.001) for RIFLE, 0.746 (P <0.001) for AKIN, and 0.757 (P <0.001) for KDIGO. KDIGO was more predictive than RIFLE for in-hospital mortality (P <0.001), but there was no difference between KDIGO and AKIN (P = 0.12).
Conclusions: A higher incidence of AKI was diagnosed according to KDIGO criteria. Patients diagnosed as AKI had a significantly higher in-hospital mortality than non-AKI patients, no matter which criteria were used. Compared with the RIFLE criteria, KDIGO was more predictive for in-hospital mortality, but there was no significant difference between AKIN and KDIGO.
Figures
References
-
- Chang CH, Lin CY, Tian YC, Jenq CC, Chang MY, Chen YC, Fang JT, Yang CW. Acute kidney injury classification: comparison of AKIN and RIFLE criteria. Shock. 2010;33:247–252. - PubMed
-
- Bagshaw SM, George C, Dinu I, Bellomo R. A multi-centre evaluation of the RIFLE criteria for early acute kidney injury in critically ill patients. Nephrol Dial Transplant. 2008;23:1203–1210. - PubMed
-
- Barrantes F, Tian J, Vazquez R, Amoateng-Adjepong Y, Manthous CA. Acute kidney injury criteria predict outcomes of critically ill patients. Crit Care Med. 2008;36:1397–1403. - PubMed
-
- Nisula S, Kaukonen KM, Vaara ST, Korhonen AM, Poukkanen M, Karlsson S, Haapio M, Inkinen O, Parviainen I, Suojaranta-Ylinen R, Laurila JJ, Tenhunen J, Reinikainen M, Ala-Kokko T, Ruokonen E, Kuitunen A, Pettilä V. FINNAKI Study Group. Incidence, risk factors and 90-day mortality of patients with acute kidney injury in Finnish intensive care units: the FINNAKI study. Intensive Care Med. 2013;39:420–428. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
