

Upfront stereotactic radiosurgery in patients with brain metastases from small cell lung cancer: retrospective analysis of 41 patients
- PMID: 25005424
- PMCID: PMC4099016
- DOI: 10.1186/1748-717X-9-152
Upfront stereotactic radiosurgery in patients with brain metastases from small cell lung cancer: retrospective analysis of 41 patients
Abstract
Background: Although the efficacy of prophylactic or therapeutic whole brain radiotherapy (WBRT) for brain metastases (BM) from small cell lung cancer (SCLC) is well established, the role of stereotactic radiosurgery (SRS) has yet to be determined. In the present retrospective analysis, we investigated whether upfront SRS might be an effective treatment option for patients with BM from SCLC.
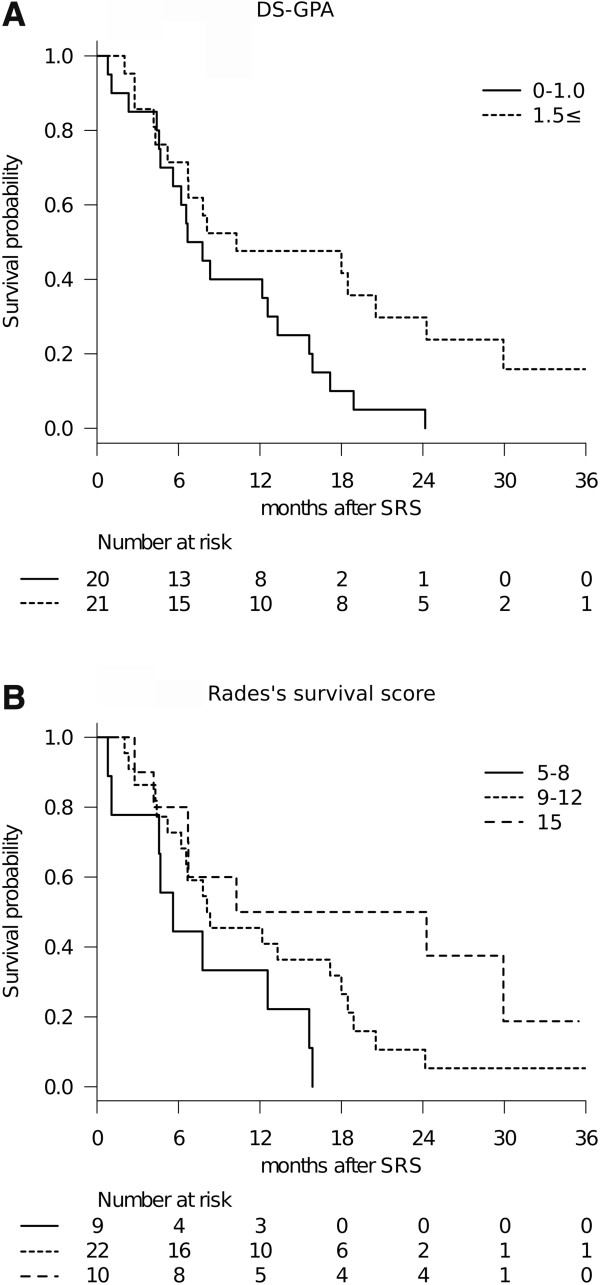
Methods: We analyzed 41 consecutive patients with a limited number of BM (≤ 10) from SCLC who received SRS as the initial treatment. No prophylactic and therapeutic WBRT was given prior to SRS. The median patient age was 69 years and the median Karnofsky performance status (KPS) score was 90. Repeat SRS was given for new distant lesions detected on follow-up neuroradiological imaging, as necessary. Overall survival, neurological death, and local and distant BM recurrence rates were analyzed. The survival results were tested with three prognostic scoring systems validated for SCLC: Diagnosis-specific graded prognostic assessment (DS-GPA), Radiation therapy oncology group -recursive partitioning analysis and Rades's survival score.
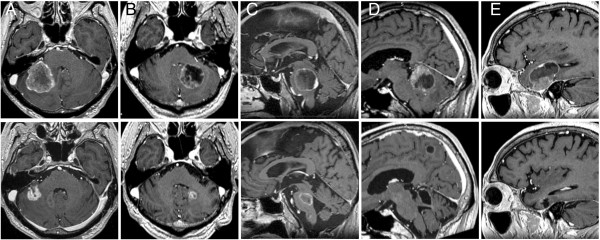
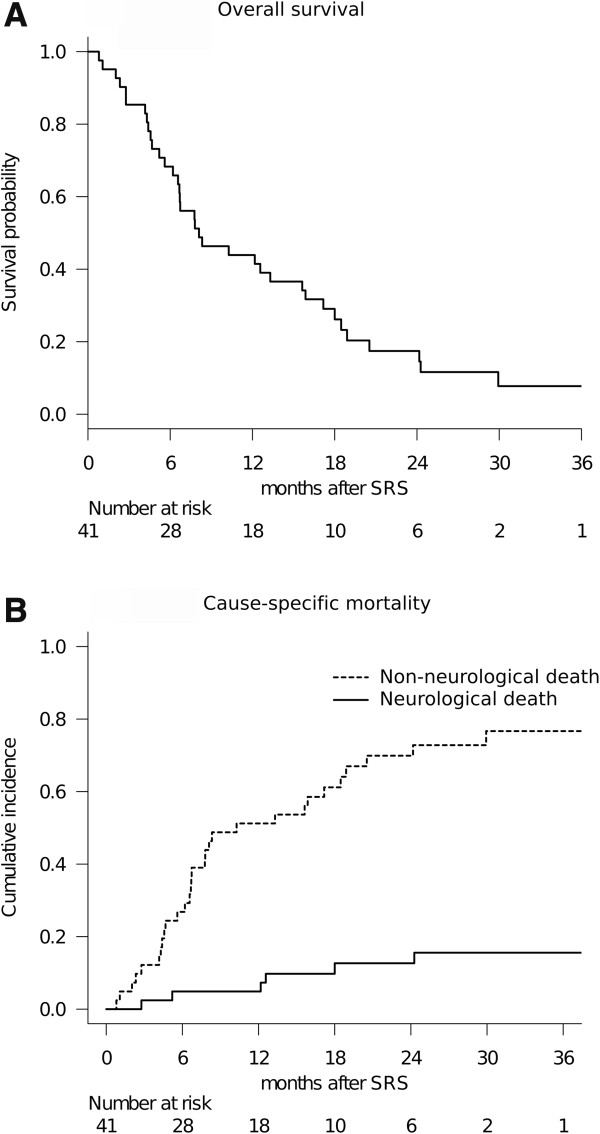
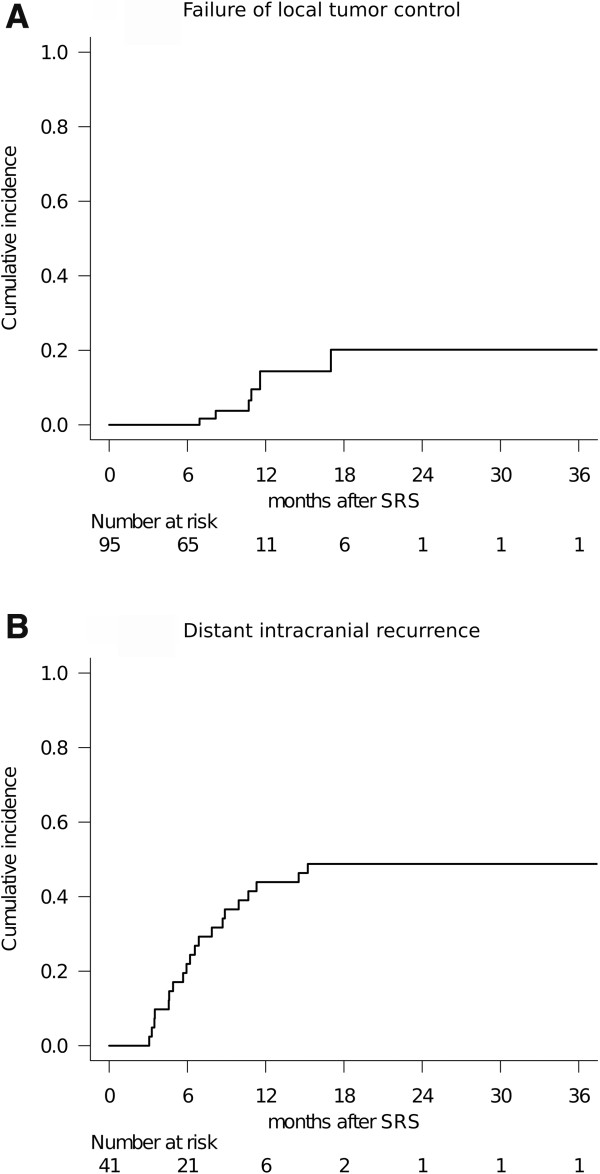
Results: One- and 2-year overall survival rates were 44% and 17%, respectively. The median survival time was 8.1 months. Survival results replicated the DS-GPA (P = 0.022) and Rades's survival score (P = 0.034). On multivariate analysis, patients with high KPS (hazard ratio (HR): 0.308, P = 0.009) and post-SRS chemotherapy (HR: 0.324, P = 0.016) had better overall survival. In total, 95/121 tumors (79%) in 34 patients (83%) with sufficient radiological follow-up data were evaluated. Six- and 12-month rates of local control failure were 0% and 14%, respectively. Six- and 12-month distant BM rates were 22% and 44%, respectively. Repeat SRS, salvage WBRT and microsurgery were subsequently required in 18, 7 and one patient, respectively. Symptomatic radiation injury developed in two patients and both were treated conservatively.
Conclusions: Our survival analyses with the validated prognostic grading systems suggested upfront SRS for limited BM from SCLC to be a potential treatment option, with patient survival being slightly more than eight months after SRS. Although SRS provided durable local tumor control, repeat treatment was needed in nearly half of patients to achieve control of distant BM.
Figures
Comment in
-
Stereotactic radiosurgery alone for small cell lung cancer: a neurocognitive benefit?Radiat Oncol. 2014 Sep 30;9:218. doi: 10.1186/1748-717X-9-218. Radiat Oncol. 2014. PMID: 25333667 Free PMC article.
Similar articles
-
Is stereotactic radiosurgery a rational treatment option for brain metastases from small cell lung cancer? A retrospective analysis of 70 consecutive patients.BMC Cancer. 2015 Mar 4;15:95. doi: 10.1186/s12885-015-1103-6. BMC Cancer. 2015. PMID: 25879433 Free PMC article.
-
Is upfront stereotactic radiosurgery a rational treatment option for very elderly patients with brain metastases? A retrospective analysis of 106 consecutive patients age 80 years and older.BMC Cancer. 2016 Dec 15;16(1):948. doi: 10.1186/s12885-016-2983-9. BMC Cancer. 2016. PMID: 27978813 Free PMC article.
-
Prognostic factors for survival in patients treated with stereotactic radiosurgery for recurrent brain metastases after prior whole brain radiotherapy.Int J Radiat Oncol Biol Phys. 2012 May 1;83(1):303-9. doi: 10.1016/j.ijrobp.2011.06.1987. Epub 2011 Nov 11. Int J Radiat Oncol Biol Phys. 2012. PMID: 22079723
-
Should Stereotactic Radiosurgery Be Considered for Salvage of Intracranial Recurrence after Prophylactic Cranial Irradiation or Whole Brain Radiotherapy in Small Cell Lung Cancer? A Population-Based Analysis and Literature Review.J Med Imaging Radiat Sci. 2020 Mar;51(1):75-87.e2. doi: 10.1016/j.jmir.2019.10.001. Epub 2019 Nov 20. J Med Imaging Radiat Sci. 2020. PMID: 31759940 Review.
-
Stereotactic radiosurgery versus whole brain radiotherapy in patients with intracranial metastatic disease and small-cell lung cancer: a systematic review and meta-analysis.Lancet Oncol. 2022 Jul;23(7):931-939. doi: 10.1016/S1470-2045(22)00271-6. Epub 2022 May 26. Lancet Oncol. 2022. PMID: 35644163
Cited by
-
Gamma Knife radiosurgery for brain metastases from small-cell lung cancer: Institutional experience over more than a decade and review of the literature.J Radiosurg SBRT. 2019;6(1):35-43. J Radiosurg SBRT. 2019. PMID: 30775073 Free PMC article.
-
Outcomes of stereotactic radiosurgery of brain metastases from neuroendocrine tumors.Neurooncol Pract. 2018 Mar;5(1):37-45. doi: 10.1093/nop/npx009. Epub 2017 May 25. Neurooncol Pract. 2018. PMID: 31385968 Free PMC article.
-
Current Management and Progress in Radiotherapy for Small Cell Lung Cancer.Front Oncol. 2020 Jul 14;10:1146. doi: 10.3389/fonc.2020.01146. eCollection 2020. Front Oncol. 2020. PMID: 32760673 Free PMC article. Review.
-
Prophylactic cranial irradiation for stage IV small cell lung cancer, live longer or reduce morbidity of brain metastases?J Thorac Dis. 2017 Oct;9(10):3572-3575. doi: 10.21037/jtd.2017.09.50. J Thorac Dis. 2017. PMID: 29268344 Free PMC article. No abstract available.
-
Brain metastases in cancer patients attending a Gamma Knife Center: A study from a single institute in Iran.Asian J Neurosurg. 2017 Jul-Sep;12(3):529-533. doi: 10.4103/1793-5482.145564. Asian J Neurosurg. 2017. PMID: 28761536 Free PMC article.
References
-
- Quan AL, Videtic GM, Suh JH. Brain metastases in small cell lung cancer. Oncology. 2004;18:961–972. discussion 974, 979-980, 987. - PubMed
-
- Castrucci WA, Knisely JP. An update on the treatment of CNS metastases in small cell lung cancer. Cancer J. 2008;14:138–146. - PubMed
-
- Arriagada R, Le Chevalier T, Borie F, Riviere A, Chomy P, Monnet I, Tardivon A, Viader F, Tarayre M, Benhamou S. Prophylactic cranial irradiation for patients with small-cell lung cancer in complete remission. J Natl Cancer Inst. 1995;87:183–190. - PubMed
-
- Auperin A, Arriagada R, Pignon JP, Le Pechoux C, Gregor A, Stephens RJ, Kristjansen PE, Johnson BE, Ueoka H, Wagner H, Aisner J. Prophylactic cranial irradiation for patients with small-cell lung cancer in complete remission. Prophylactic Cranial Irradiation Overview Collaborative Group. N Engl J Med. 1999;341:476–484. - PubMed
-
- D'Ambrosio DJ, Cohen RB, Glass J, Konski A, Buyyounouski MK, Feigenberg SJ. Unexpected dementia following prophylactic cranial irradiation for small cell lung cancer: case report. J Neurooncol. 2007;85:77–79. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
