

Evidence for mTOR pathway activation in a spectrum of epilepsy-associated pathologies
- PMID: 25005575
- PMCID: PMC4230418
- DOI: 10.1186/2051-5960-2-71
Evidence for mTOR pathway activation in a spectrum of epilepsy-associated pathologies
Abstract
Introduction: Activation of the mTOR pathway has been linked to the cytopathology and epileptogenicity of malformations, specifically Focal Cortical Dysplasia (FCD) and Tuberous Sclerosis (TSC). Experimental and clinical trials have shown than mTOR inhibitors have anti-epileptogenic effects in TS. Dysmorphic neurones and balloon cells are hallmarks of FCDIIb and TSC, but similar cells are also occasionally observed in other acquired epileptogenic pathologies, including hippocampal sclerosis (HS) and Rasmussen's encephalitis (RE). Our aim was to explore mTOR pathway activation in a range of epilepsy-associated pathologies and in lesion-negative cases.
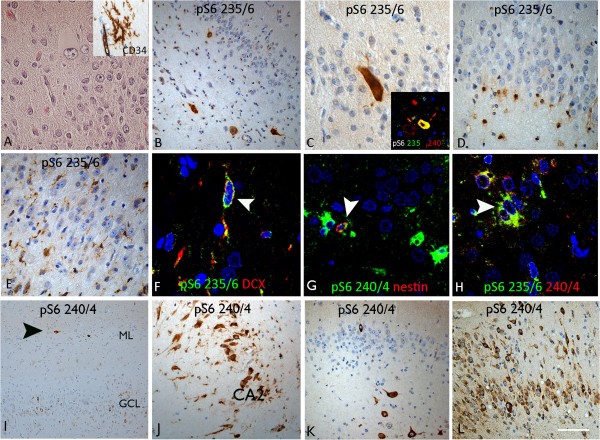
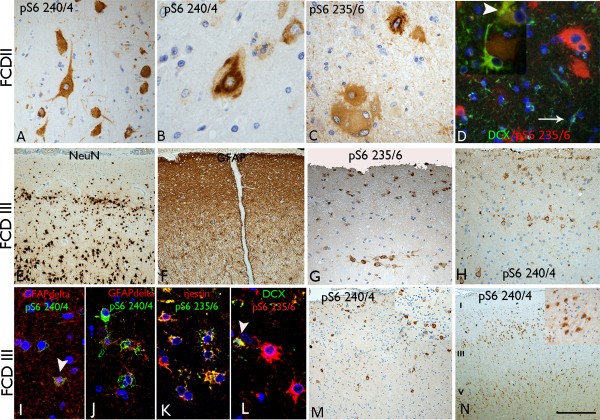
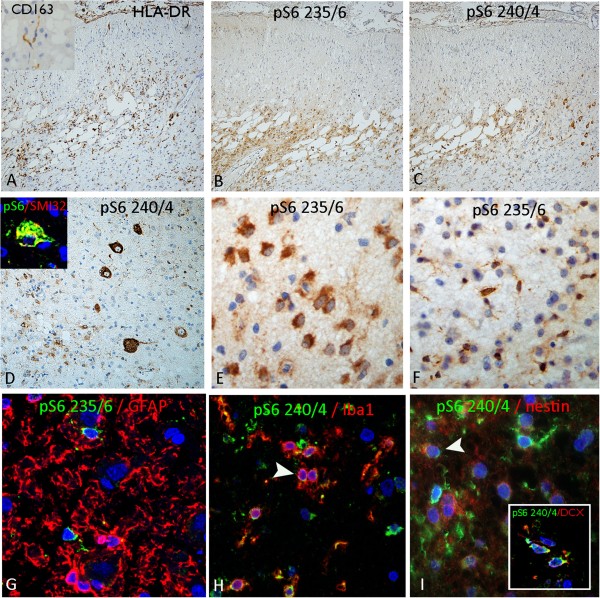
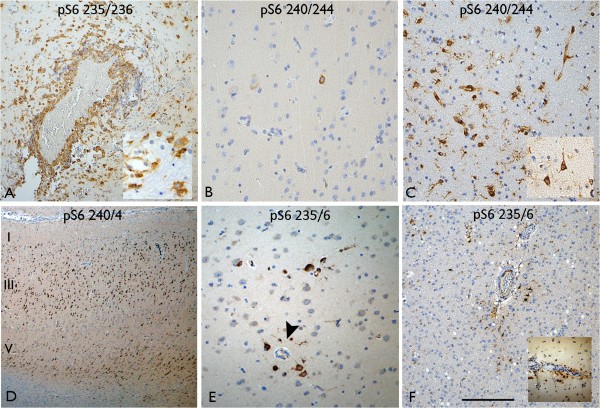
Results: 50 epilepsy surgical pathologies were selected including HS ILAE type 1 with (5) and without dysmorphic neurones (4), FCDIIa (1), FCDIIb (5), FCDIIIa (5), FCDIIIb (3), FCDIIId (3), RE (5) and cortex adjacent to cavernoma (1). We also included pathology-negative epilepsy cases; temporal cortex (7), frontal cortex (2), paired frontal cortical samples with different ictal activity according to intracranial EEG recordings (4), cortex with acute injuries from electrode tracks (5) and additionally non-epilepsy surgical controls (3). Immunohistochemistry for phospho-S6 (pS6) ser240/244 and ser235/236 and double-labelling for Iba1, neurofilament, GFAP, GFAPdelta, doublecortin, and nestin were performed. Predominant neuronal labelling was observed with pS6 ser240/244 and glial labelling with pS6 ser235/236 in all pathology types but with evidence for co-expression in a proportion of cells in all pathologies. Intense labelling of dysmorphic neurones and balloon cells was observed in FCDIIb, but dysmorphic neurones were also labelled in RE and HS. There was no difference in pS6 labelling in paired samples according to ictal activity. Double-labelling immunofluorescent studies further demonstrated the co-localisation of pS6 with nestin, doublecortin, GFAPdelta in populations of small, immature neuroglial cells in a range of epilepsy pathologies.
Conclusions: Although mTOR activation has been more studied in the FCDIIb and TSC, our observations suggest this pathway is activated in a variety of epilepsy-associated pathologies, and in varied cell types including dysmorphic neurones, microglia and immature cell types. There was no definite evidence from our studies to suggest that pS6 expression is directly related to disease activity.
Figures
Similar articles
-
FCD Type II and mTOR pathway: Evidence for different mechanisms involved in the pathogenesis of dysmorphic neurons.Epilepsy Res. 2017 Jan;129:146-156. doi: 10.1016/j.eplepsyres.2016.12.002. Epub 2016 Dec 7. Epilepsy Res. 2017. PMID: 28056425
-
Doublecortin-expressing cell types in temporal lobe epilepsy.Acta Neuropathol Commun. 2018 Jul 13;6(1):60. doi: 10.1186/s40478-018-0566-5. Acta Neuropathol Commun. 2018. PMID: 30005693 Free PMC article.
-
mTOR pathway activation in focal cortical dysplasia.Ann Diagn Pathol. 2020 Jun;46:151523. doi: 10.1016/j.anndiagpath.2020.151523. Epub 2020 Apr 10. Ann Diagn Pathol. 2020. PMID: 32325422
-
Cortical Dysplasia and the mTOR Pathway: How the Study of Human Brain Tissue Has Led to Insights into Epileptogenesis.Int J Mol Sci. 2022 Jan 25;23(3):1344. doi: 10.3390/ijms23031344. Int J Mol Sci. 2022. PMID: 35163267 Free PMC article. Review.
-
Mammalian target of rapamycin (mTOR) activation in focal cortical dysplasia and related focal cortical malformations.Exp Neurol. 2013 Jun;244:22-6. doi: 10.1016/j.expneurol.2011.10.002. Epub 2011 Oct 8. Exp Neurol. 2013. PMID: 22015915 Free PMC article. Review.
Cited by
-
mTOR inhibition in epilepsy: rationale and clinical perspectives.CNS Drugs. 2015 Feb;29(2):91-9. doi: 10.1007/s40263-014-0223-x. CNS Drugs. 2015. PMID: 25633849 Free PMC article. Review.
-
Rodent Models of Audiogenic Epilepsy: Genetic Aspects, Advantages, Current Problems and Perspectives.Biomedicines. 2022 Nov 15;10(11):2934. doi: 10.3390/biomedicines10112934. Biomedicines. 2022. PMID: 36428502 Free PMC article. Review.
-
The Glucagon-Like Peptide-1 Analogue Liraglutide Reduces Seizures Susceptibility, Cognition Dysfunction and Neuronal Apoptosis in a Mouse Model of Dravet Syndrome.Front Pharmacol. 2020 Feb 28;11:136. doi: 10.3389/fphar.2020.00136. eCollection 2020. Front Pharmacol. 2020. PMID: 32184723 Free PMC article.
-
Caloric Restriction and Ketogenic Diet Therapy for Epilepsy: A Molecular Approach Involving Wnt Pathway and KATP Channels.Front Neurol. 2020 Nov 5;11:584298. doi: 10.3389/fneur.2020.584298. eCollection 2020. Front Neurol. 2020. PMID: 33250850 Free PMC article. Review.
-
WONOEP appraisal: The role of glial cells in focal malformations associated with early onset epilepsies.Epilepsia. 2024 Dec;65(12):3457-3468. doi: 10.1111/epi.18126. Epub 2024 Oct 14. Epilepsia. 2024. PMID: 39401070 Free PMC article. Review.
References
-
- Blumcke I, Thom M, Aronica E, Armstrong DD, Vinters HV, Palmini A, Jacques TS, Avanzini G, Barkovich AJ, Battaglia G, Becker A, Cepeda C, Cendes F, Colombo N, Crino P, Cross JH, Delalande O, Dubeau F, Duncan J, Guerrini R, Kahane P, Mathern G, Najm I, Ozkara C, Raybaud C, Represa A, Roper SN, Salamon N, Schulze-Bonhage A, Tassi L, et al. The clinicopathologic spectrum of focal cortical dysplasias: a consensus classification proposed by an ad hoc task force of the ILAE diagnostic methods commission. Epilepsia. 2011;52(1):158–174. doi: 10.1111/j.1528-1167.2010.02777.x. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
