

Outcomes after treatment of 17,378 patients with locally advanced (T3N0-2) non-small-cell lung cancer
- PMID: 25005840
- PMCID: PMC4366575
- DOI: 10.1093/ejcts/ezu270
Outcomes after treatment of 17,378 patients with locally advanced (T3N0-2) non-small-cell lung cancer
Abstract
Objectives: Treatment patterns and outcomes in a population-based database were examined to identify patients likely to benefit from surgical resection of locally advanced (T3N0-2) non-small-cell lung cancer (NSCLC).
Methods: Factors predicting the use of surgery for patients with T3N0-2M0 NSCLC in the Surveillance, Epidemiology and End Results (SEER) database from 1988 to 2010 were assessed using a multivariable logistic regression model. Survival was analysed using the Kaplan-Meier approach and Cox proportional hazard models. Propensity matching was used to compare outcomes after surgery and outcomes in patients who refused surgery and underwent radiation therapy (RT).
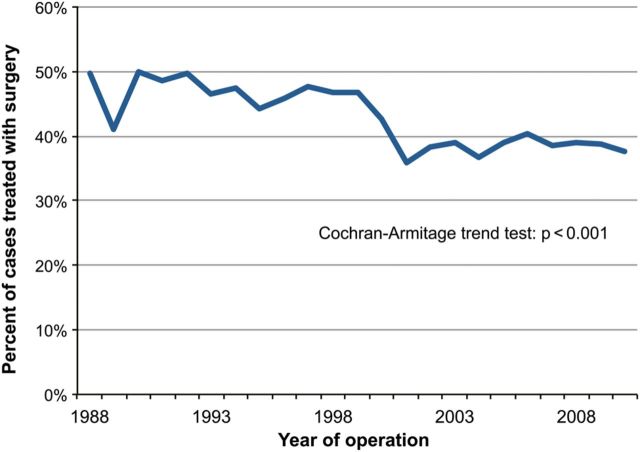
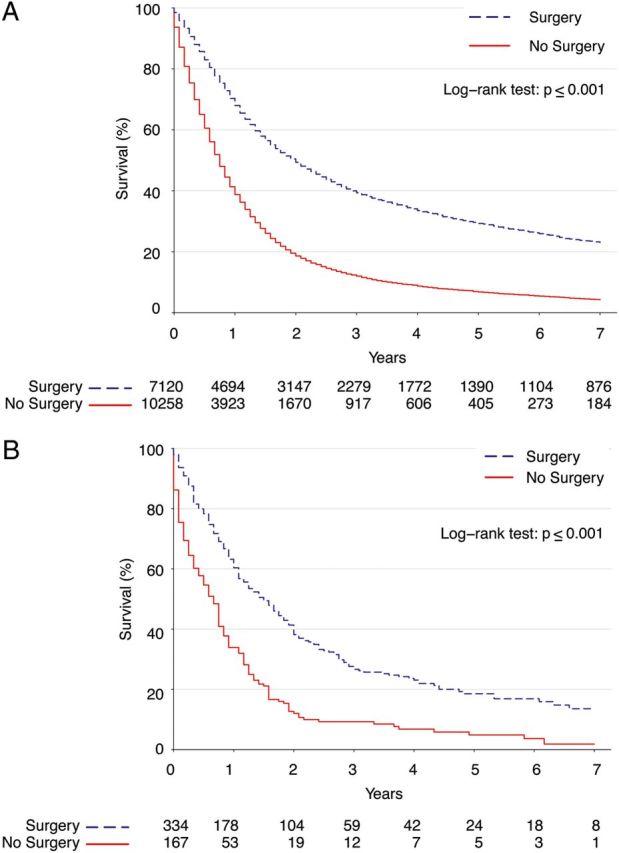
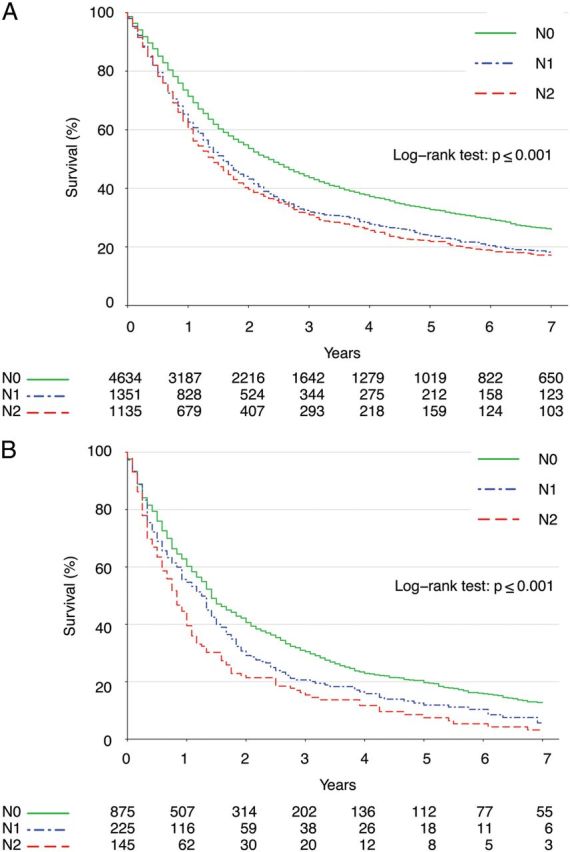
Results: Of 17 378 patients identified for study inclusion [8597 (50%) T3N0, 2304 (13%) T3N1 and 6477 (37%) T3N2], surgery was used in 7120 (41%). Only female sex and being married predicted the use of surgery, while older age, black race and N2 nodal disease predicted non-surgical management. Surgical patients overall had better long-term survival than non-surgical patients [odds ratio (OR) 0.42, 95% confidence interval (CI): 0.41-0.45, P < 0.001]. After propensity adjustment, patients who refused surgery and instead were treated with RT had significantly worse long-term survival than matched surgery patients (OR 0.65, 95% CI: 0.48-0.89, P = 0.0074). Sublobar resection and pneumonectomy predicted worse survival in patients who had surgery. Nodal disease also predicted worse survival after surgery, but surgery maintained an association with better overall survival compared with non-operative therapy among patients with both N1 (OR 0.53, P < 0.001) and N2 disease (OR 0.50, P < 0.001) in separate analyses stratified by nodal status. Older age also predicted worse survival after surgery, but patients older than 75 who were treated with surgery had significantly better long-term survival than non-operative patients (OR 0.49, 95% CI: 0.45-0.53, P < 0.001).
Conclusions: Surgery is used in a minority of patients with locally advanced NSCLC, but is associated with better survival than non-surgical treatment, even for patients older than 75 and patients with nodal disease. Given the very poor outcomes observed with non-operative management, surgical resection should be carefully considered in all patients with locally advanced NSCLC and should not necessarily be denied because of patient age or nodal disease.
Keywords: Chest wall; Lobectomy; Lung cancer surgery; Outcomes; Pneumonectomy.
© The Author 2014. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
Figures
Similar articles
-
Impact of preoperative radiation on survival of patients with T3N0 >7-cm non-small cell lung cancers treated with anatomic resection using the Surveillance, Epidemiology, and End Results database.J Surg Res. 2013 Sep;184(1):10-8. doi: 10.1016/j.jss.2013.03.053. Epub 2013 Apr 3. J Surg Res. 2013. PMID: 23583079
-
Thoracoscopic lobectomy is associated with improved short-term and equivalent oncological outcomes compared with open lobectomy for clinical Stage I non-small-cell lung cancer: a propensity-matched analysis of 963 cases.Eur J Cardiothorac Surg. 2014 Oct;46(4):607-13. doi: 10.1093/ejcts/ezu036. Epub 2014 Mar 5. Eur J Cardiothorac Surg. 2014. PMID: 24603446
-
Lobectomy, sublobar resection, and stereotactic ablative radiotherapy for early-stage non-small cell lung cancers in the elderly.JAMA Surg. 2014 Dec;149(12):1244-53. doi: 10.1001/jamasurg.2014.556. JAMA Surg. 2014. PMID: 25321323 Free PMC article.
-
A review of 250 ten-year survivors after pneumonectomy for non-small-cell lung cancer.Eur J Cardiothorac Surg. 2014 May;45(5):876-81. doi: 10.1093/ejcts/ezt494. Epub 2013 Oct 16. Eur J Cardiothorac Surg. 2014. PMID: 24132299 Review.
-
Multimodality Treatment including Surgery Related to the Type of N2 Involvement in Locally Advanced Non-Small Cell Lung Cancer.Cancers (Basel). 2022 Mar 25;14(7):1656. doi: 10.3390/cancers14071656. Cancers (Basel). 2022. PMID: 35406428 Free PMC article. Review.
Cited by
-
125I Brachytherapy in Locally Advanced Nonsmall Cell Lung Cancer After Progression of Concurrent Radiochemotherapy.Medicine (Baltimore). 2015 Dec;94(49):e2249. doi: 10.1097/MD.0000000000002249. Medicine (Baltimore). 2015. PMID: 26656370 Free PMC article.
-
Non-small cell lung cancer with pathological complete response: predictive factors and surgical outcomes.Gen Thorac Cardiovasc Surg. 2019 Sep;67(9):773-781. doi: 10.1007/s11748-019-01076-9. Epub 2019 Feb 6. Gen Thorac Cardiovasc Surg. 2019. PMID: 30725275
-
Oncological outcomes from trimodality therapy receiving definitive doses of neoadjuvant chemoradiation (≥60 Gy) and factors influencing consideration for surgery in stage III non-small cell lung cancer.Adv Radiat Oncol. 2017 Jul 31;2(3):259-269. doi: 10.1016/j.adro.2017.07.009. eCollection 2017 Jul-Sep. Adv Radiat Oncol. 2017. PMID: 29114590 Free PMC article.
-
Robotic versus Open Surgery in Locally Advanced Non-Small Cell Lung Cancer: Evaluation of Surgical and Oncological Outcomes.Curr Oncol. 2023 Oct 12;30(10):9104-9115. doi: 10.3390/curroncol30100658. Curr Oncol. 2023. PMID: 37887558 Free PMC article.
-
Trends in use and safety of image-guided transthoracic needle biopsies in patients with cancer.J Oncol Pract. 2015 May;11(3):e351-9. doi: 10.1200/JOP.2014.001891. Epub 2015 Jan 20. J Oncol Pract. 2015. PMID: 25604594 Free PMC article.
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- Howlader N, Noone AM, Krapcho M, Garshell J, Neyman N, Altekruse SF, et al. SEER Cancer Statistics Review, 1975–2010. Bethesda, MD: National Cancer Institute; 2013. http://seer.cancer.gov/csr/1975_2010/ based on November 2012 SEER data submission, posted to the SEER web site, April.
-
- Ettinger DS, Akerley W, Borghaei H, Chang AC, Cheney RT, Chirieac LR, et al. Non-small cell lung cancer, version 2.2013. J Natl Compr Canc Netw. 2013;11:645–53. - PubMed
-
- Kozower BD, Larner JM, Detterbeck FC, Jones DR. Special treatment issues in non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143:e369S–99S. - PubMed
-
- Pisters KM, Evans WK, Azzoli CG, Kris MG, Smith CA, Desch CE, et al. Cancer Care Ontario and American Society of Clinical Oncology adjuvant chemotherapy and adjuvant radiation therapy for stages I-IIIA resectable non small-cell lung cancer guideline. J Clin Oncol. 2007;25:5506–18. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
